Papillary hidradenoma (hidradenoma papilliferum)
Papillary hidradenoma (hidradenoma papilliferum)
Clinical features Papillary hidradenoma (hidradenoma papilliferum) occurs almost exclusively in females.1,2 A single example of a perianal variant has been described in a male.3 The age range is wide, with tumors presenting in adult females with a predilection for the fifth and sixth decades of life.
Papillary hidradenoma typically presents as a small (1–2 cm diameter) solitary asymptomatic nodule in a vulval, perineal, or perianal location.4,5 Rare lesions attain a large size.6 Lesions may present with bleeding or pruritus and rarely ulcerated. Most often it affects the labium majus, but on occasion it arises on the lateral aspect of the labium minus, fourchette, or clitoris (Fig. 12.272), and is seen at the sites of anogenital mammary-like glands.5,7 Perianal lesions are very uncommon.8 Rarely, tumors are multiple and such cases tend to be located on the same side of the vulva.1 Very rarely, lesions have been described on the nipple, eyelid, and external auditory canal.9,10
The epidermis may be normal, acanthotic, or ulcerated. A connection to the epidermis, and less commonly to the infundibulae of hair follicles, may be seen. In such cases, tumors resemble syringocystadenoma papilliferum, even displaying prominent plasma cells in the stroma.11,15 The tumor forms a fairly well-demarcated nodule in the dermis or lamina propria and sometimes shows foci of continuity with the overlying epithelium. The growth pattern consists of a mixture of tubular, papillary, and solid areas.4 It is composed of epithelium-covered papillary processes projecting into cystic spaces (Fig. 12.273). Cystic change, sometimes prominent, is seen in a small percentage of cases The epithelial lining is typically double layered, comprising outer small myoepithelial cells with oval hyperchromatic nuclei and inner tall columnar cells with eosinophilic cytoplasm, often manifesting decapitation secretion, indicating apocrine lineage (Figs 12.274 and 12.275). Cytological atypia is mild or absent. Squamous and mucinous metaplasia are very rarely identified.11 Oxyphilic metaplasia of tumor cells is common, and tumor cells display more cytological atypia and a single prominent nucleolus.16 Tumor cells are epithelial and myoepithelial, and the latter can display clear cell change.4 Clear cell change in epithelial cells (lamprocytes) is very rare.11 Occasionally, the lining is only one cell thick (columnar). Diastase-resistant, PAS-positive intracytoplasmic granules are usually present. The occasional finding of a normal mitotic figure has no sinister implication. The larger villi have a fibrous core in which occasional ductal structures may be identified. Often, the fibrous tissue surrounding the tumor is compressed to form a pseudocapsule. Some tumors have a pattern
Pathogenesis and histologic features This tumor is likely to be derived from anogenital mammary-like glands, and although the name mammary-like gland adenoma of the vulva has been proposed this has not been universally accepted.4 The lesion is the equivalent of mammary intraductal papilloma.11,12 The close relationship between tumors is further given support by a similar immunohistochemical profile and mutations in both neoplasms.11,13,14 The latter include PIK3CA and AKT1 mutations.13,14
548 Diseases of the anogenital skin
identical to those of breast tumors including erosive adenomatosis, sclerosing adenosis, and ductal hyperplasia.4 An inflammatory cell component is not a significant feature except in ulcerated lesions and those connected to the overlying epithelium, but foamy histiocytes can be seen. In the surrounding stroma, residual anogenital mammary-like glands are found and may display hyperplasia.11
Very rarely, coexistence with extramammary Paget is noted.11 Exceptionally rarely, a malignant variant has been reported.16–18 The diagnosis of a handful of invasive cases reported in the literature including one described as an adenosquamous carcinoma, has been challenged and so far only cases of carcinoma in situ developing within the tumors have been accepted as genuine. In these cases, involved glands are associated with an intact layer of pericytes. In a single case, association with HPV16 was reported.
HPV has only occasionally been detected in this tumor, but this is not likely to have an etiological link.19
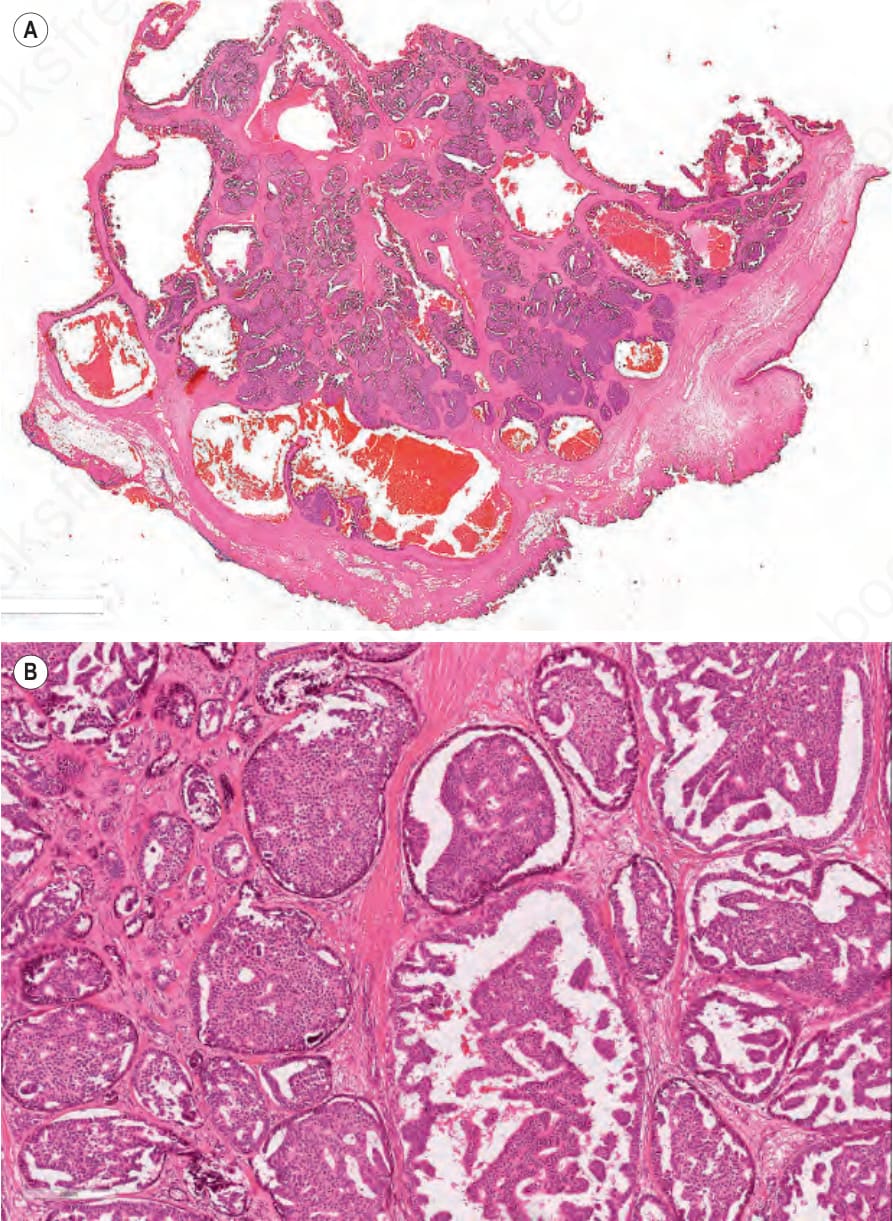
Fig. 12.271 (A, B). Adenocarcinoma of anogenital mammary-type glands: low- and high-power views highlighting the similarities to breast adenocarcinoma. By courtesy of Dr Catherine Stefanato, St John’s Institute of Dermatology, London, UK.

Fig. 12.272 Papillary hidradenoma: the lesion presents as a warty nodule. By courtesy of the Institute of Dermatology, London, UK.
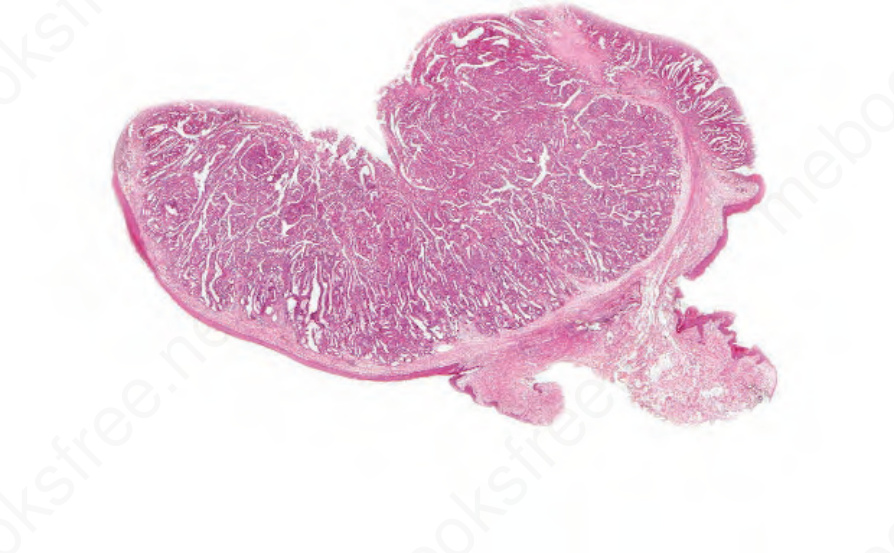
Fig. 12.273 Papillary hidradenoma: whole mount preparation showing sharply circumscribed papillary tumor.
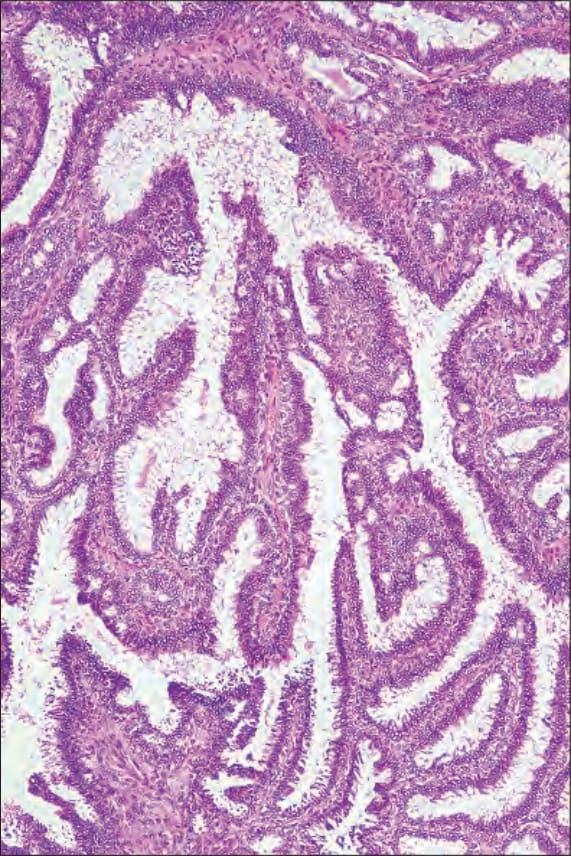
Fig. 12.274 Papillary hidradenoma: the papillae have a fibrovascular core.
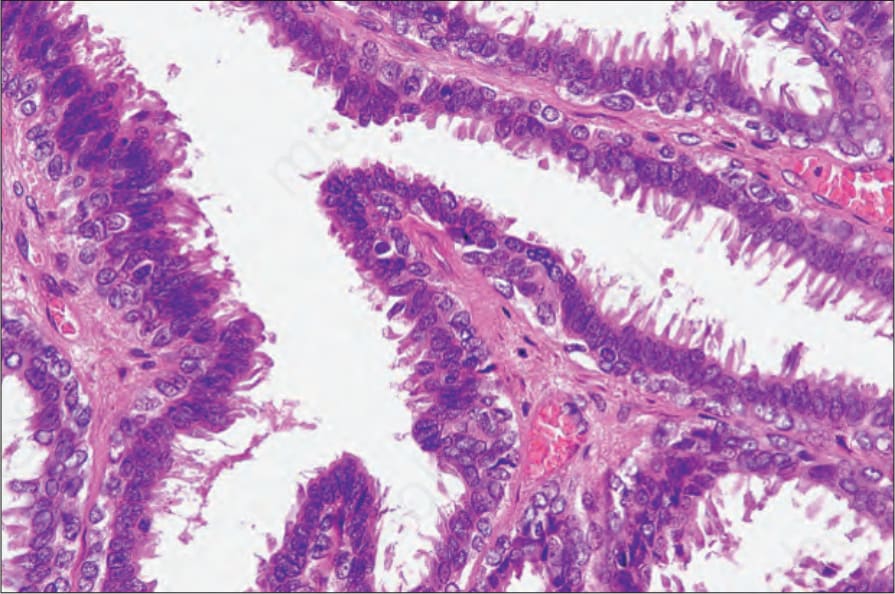
Fig. 12.275 Papillary hidradenoma: the papillae are covered by a double layer of epithelial cells, the inner showing typical decapitation secretion.