Melanoma
Melanoma
Clinical features Genitourinary melanoma is rare but 10 times more common in women than men in the United States.1,2 Female genital melanoma accounts for around 3% of all female melanomas and 2–10% of female genital tract malignancies.3,4 Mucosal female tract melanomas account for 18% of all mucosal melanomas. The vulva is the most frequently involved site followed by the vagina and much less often the cervix (Fig. 12.164).5 The labia majora and the clitoris are the most commonly affected sites. Most patients present in the sixth and seventh decades of life. Less than one-third of cases occur in patients younger than 50 years of age. Melanoma of the vulva in children is exceptional and in some cases reported in association with LS.6 An association with melanosis is very rare,7 and a tumor in a young woman, a frequent user of tanning parlors, has been documented.8
Clinical presentation varies from flat to raised polypoid brown to black lesions. Ulceration may be present. Less commonly, patients complain of pruritus and/or bleeding. Amelanotic melanomas are reported to be rare, but they represented 27% of all cases in a large Swedish series.4–9 They may clinically mimic SCC or extramammary Paget disease.
Some tumors arise within a preexisting nevus. A recent study found the latter to occur in around 5% of cases.4 Most of these are of the superficial spreading type.
519 Genital pigmentation
A
B
A recent study reports a 45% 5-year survival rate for patients with vulval melanoma, which is 15% lower than matched controls with cutaneous melanoma.10 As with melanomas presenting elsewhere, tumor thickness is the best predictor of survival.3,11 Staging has also been found to be an independent predictor of survival. In addition, in stage I disease only, ulceration and the presence of clinical amelanosis were found to be independent predictors of survival.12 Radical surgery for vulval melanoma does not seem to influence outcome. A multivariate analysis of 644 patients with vulval melanoma found that young age, localized disease, and negative lymph nodes were independent prognostic factors.10 The 5-year disease-specific survival was 75.5%, 38.7%, and 22.1% for patients with localized, regional, and distant disease, respectively.
Melanoma of the male genital skin is very rare, as are those arising around or on the anus (Fig. 12.165).13–16 Penile metastasis of cutaneous melanoma elsewhere is exceptional.17 The most common site in men is the glans, but rare cases may present elsewhere, including the shaft and the
520 Diseases of the anogenital skin
scrotum.18–20 The diagnosis can be delayed because of the patient’s reluctance to seek medical help.21 Exceptional cases complicating penile melanosis, penile nevi, have been reported, also a penile melanoma which developed simultaneously with SCC.22–24 Because of the rarity of the disease, estimation of prognosis is difficult. In the few cases reported, the prognosis appears poor but this seems to be related to late presentation, delay in diagnosis, and problems in achieving complete clearance because of the site. A study of a series of 19 primary mucosal penile melanomas and a review of 47 cases reported in the literature found 2- and 5-year survival rates of 63% and 31%, respectively25 All patients presenting with nodal and/or distant metastasis died of disease within 2 years.26 The prognosis is similar in patients who present with metastatic disease on the penis from a primary tumor elsewhere.25 Poor prognosis was associated with ulceration, Breslow thickness of more than 3.5 mm, and a tumor diameter of more than 15 mm. The behavior of mucosal penile melanoma appears to be the same as cutaneous melanoma elsewhere of similar thickness.
Pathogenesis and histologic features Unlike cutaneous melanoma, it is difficult to postulate a major role for ultraviolet radiation in genital melanomagenesis. However, a case of melanoma in situ of the glans has been reported in a naturist with a short prepuce.27 A significant number of mucosal melanomas have shown mutations in c-kit as opposed to melanomas arising in skin exposed intermittently to the sun, in which BRAF mutations are frequently found.28–30 Somatic mutations in P53 are also often seen in genital melanomas.30 The presence of c-kit mutations offers the possibility of targeted therapy to those melanomas harboring the mutation. A study of vulvar and vaginal melanomas detected HPV-3 and epidermodysplasia verruciformis-associated types of HPV in a number of lesions.31 Since these HPV types are not usually found in the vulva or vagina, it has been suggested that they may play a role in the pathogenesis of melanomas at these sites.
Histologic features of genital melanoma are identical to melanomas elsewhere. Until recently, there was no consensus as to the most common type of genital melanoma. Recently, however, a large study found that 57% of vulval melanomas were mucosal lentiginous, 22% nodular, 12% unclassified, and 4% superficial spreading.32 Desmoplastic and neurotropic variants may also occasionally be encountered. Multiple in situ penile melanomas have been documented.33
foam cells.3,4 An association with squamous carcinoma5 has been reported, but HPV is not implicated in the pathogenesis of verruciform xanthoma.6
In females, an association with LS and other inflammatory conditions has been suggested.7
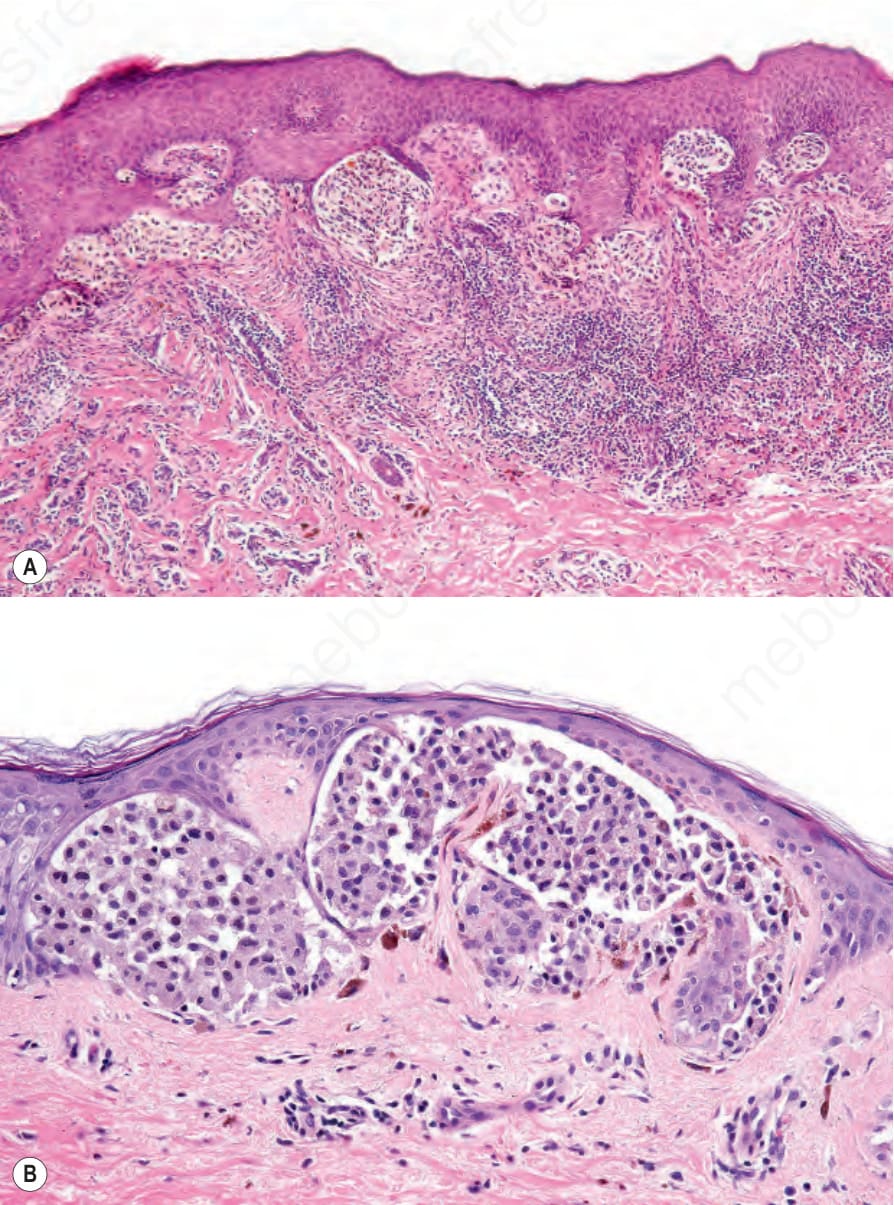
Fig. 12.160 (A, B) Atypical genital-type nevus: in this example, the junctional nests are large and due to fine melanin pigmentation; the cytoplasm has a grayish hue. Note the nuclear hyperchromatism.
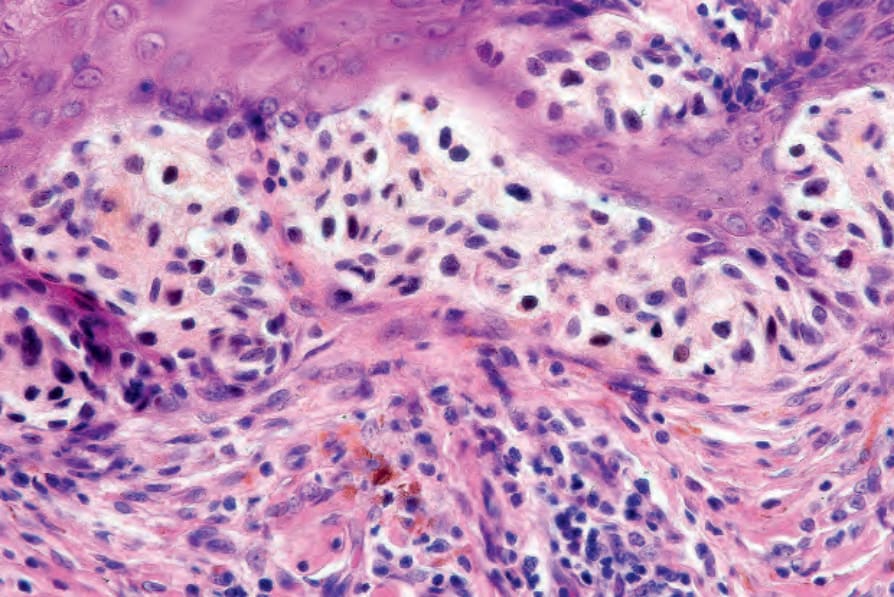
Fig. 12.161 Atypical genital-type nevus: in this field, there is nuclear hyperchromatism and mild pleomorphism.
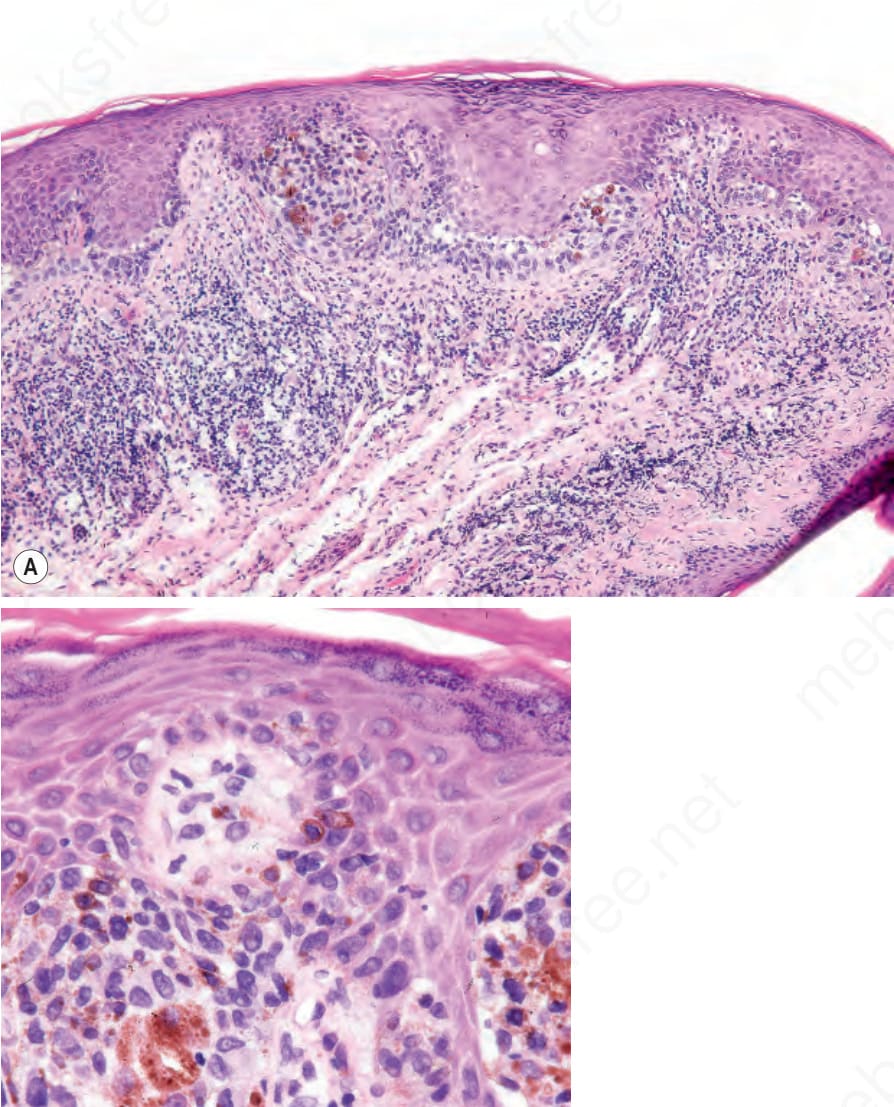
Fig. 12.162 (A, B) Atypical genital-type nevus: this example from the vulva of a 20-year-old female shows severe cytological atypia. The biological behavior of this nevus variant is uncertain although the likelihood of malignancy is very low. It should, however, be completely excised.

Fig. 12.163 Divided or ‘kissing’ nevus: note the pigmented lesions on the shaft and the glans penis. From Bunker C. Male Genital Skin Disease. Saunders Ltd./Elsevier 2004.

Fig. 12.164 Vulval melanoma: tumors at this site are very rare. They are commonly thick at presentation and therefore generally associated with a poor prognosis. By courtesy of M. Ridley, MD, Institute of Dermatology, London, UK.

Fig. 12.165 Penile melanoma: note the large size, irregular border, and variable pigmentation. By courtesy of the Institute of Dermatology, London, UK.

Fig. 12.166 Verruciform xanthoma of the vulva: warty plaque on right labium majus with lichen sclerosus