Genital melanosis
Genital melanosis
Histologic features Genital melanosis is characterized by increased pigmentation of basal keratinocytes and melanocytes (Fig. 12.155). By definition, there is no increase in melanocyte number. If, however, melanocytes are present in increased numbers, the term ‘genital lentiginosis’ may be more appropriate.16 In real terms, the difference is academic. There is no evidence of junctional activity
Clinical features Genital melanosis is characterized by pigmentation with no overt evidence of a preceding inflammatory dermatosis.1–5 However, in men the clinical suspicion is usually raised of past or chronic low-grade LS, LP, ZB, or non-specific balanoposthitis. The pigmentation may vary in its intensity and is typically irregular. The problem usually affects several sites including cutaneous and mucosal surfaces. The pigmentation develops slowly and can be very extensive. In most cases of genital melanosis, lesions become stable and may regress.6
Unifocal lesions can also sometimes occur. Small discrete single or multiple lesions are usually described as genital melanotic macules.4 The most common sites are the glans and shaft of the penis and the inner aspects of the vulva including the vestibule (Figs 12.153 and 12.154). Lesions may also affect the vagina and cervix.7,8
The condition is considered benign, but there are rare anecdotal reports of melanoma ensuing in areas of melanosis.9,10 Melanoma rarely occurs in the context of vulval melanosis, and this is likely because in the latter condition there is no increase in the number of melanocytes but only basal cell layer hyperpigmentation. Penile lesions, on the other hand, often display an
517 Genital pigmentation
and, in most cases, cytological atypia is absent. However, it has been suggested that in lesions with increased number of melanocytes and any degree of cytological atypia, there may be an association with melanomas elsewhere in the skin.6 Pigment-laden macrophages may be conspicuous in the underlying dermis. An important pitfall is the presence of coexistent LS, as the dermal changes may mimic a completely regressed melanoma.17
The histologic features of Dowling-Degos disease are specific: moderate orthokeratosis or hyperkeratosis, thinning of the suprapapillary epithelium, ‘antler-like’ branching of the rete ridges, basal pigmentation with no increase in melanocytic number (S100 normal).18
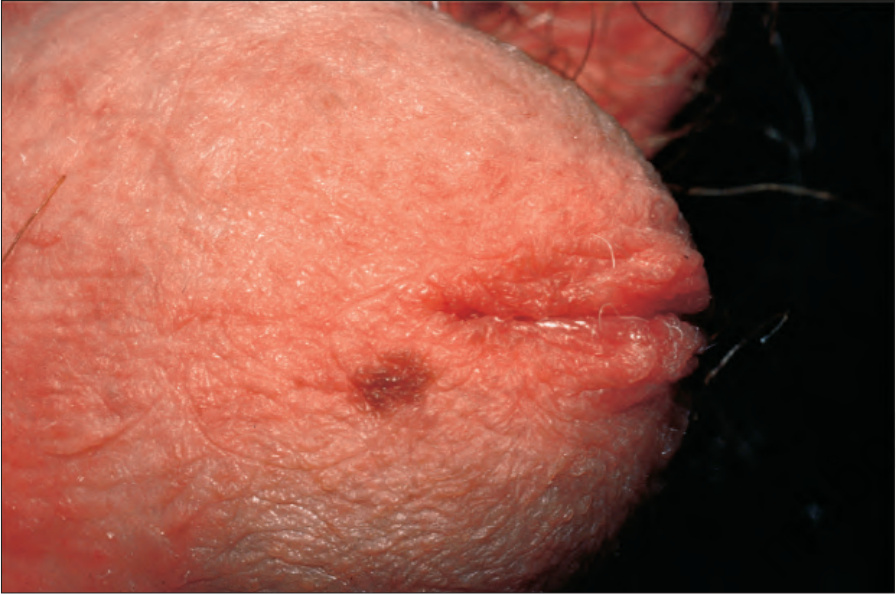
Fig. 12.153 Penile melanotic macule: there is a small irregular pigmented macule on the glans penis. By courtesy of the Institute of Dermatology, London, UK.

Fig. 12.154 Vulval melanosis: there are multiple irregular pigmented macules on the vulva and adjacent skin. By courtesy of the Institute of Dermatology, London, UK.
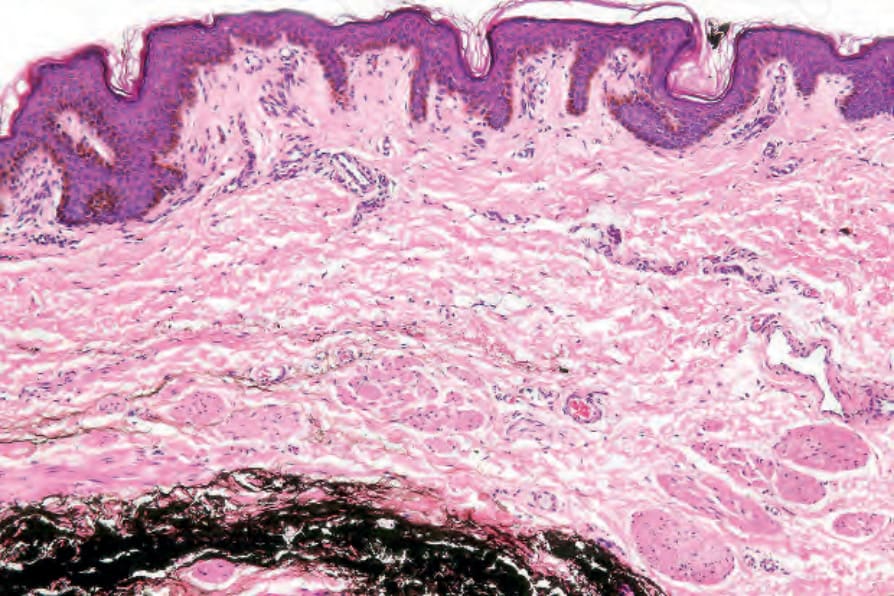
Fig. 12.155 Vulval melanosis: there is marked basal cell pigmentation.

Fig. 12.156 Atypical vulval nevus: there is an irregular darkly pigmented lesion on the perineum. By courtesy of the Institute of Dermatology, London, UK.
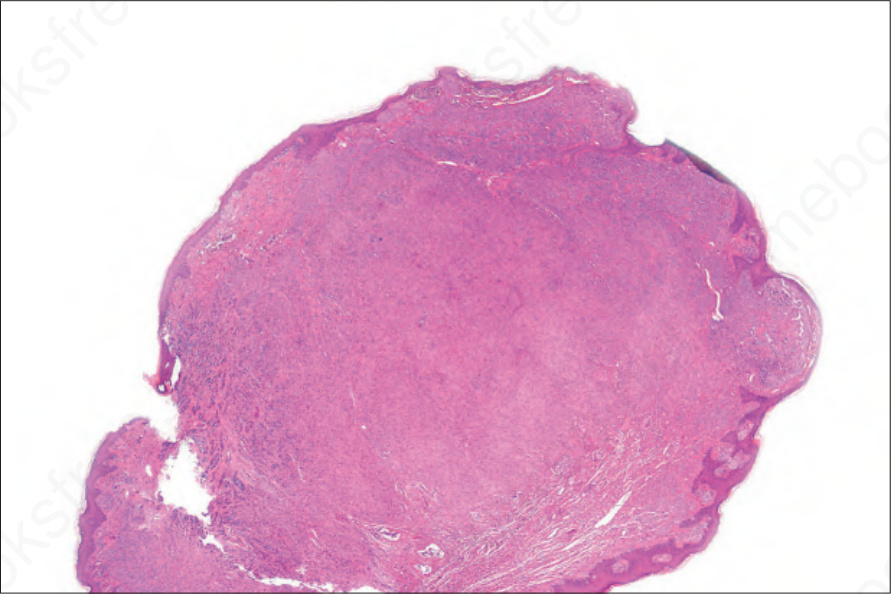
Fig. 12.157 Atypical vulval nevus: scanning view of a polypoid lesion from a 17-year-old female. Note the heavily pigmented nests at the top of the field. By courtesy of the Institute of Dermatology, London, UK.