Fournier gangrene
Fournier gangrene
Fournier gangrene is analogous to necrotizing fasciitis and Meleney gangrene. The disease begins with urethral or appendageal polybacterial infection. Most of the organisms isolated are resident urethral or lower gastrointestinal flora, and most patients have mixed infections. In children, staphylococci and streptococci are most commonly isolated.1 A necrotizing
514 Diseases of the anogenital skin
vasculitis is initiated that involves skin, subcutis, fascia, and muscle. Classically painful erythematous swelling of the genitals occurs (particularly the scrotum,2 where a dark red or a black spot may appear) that spreads to perianal or lower abdominal skin, and there may be urinary retention.3 There is crepitus but no suppuration.4 In adults there is systemic toxicity, but this may be absent in children.3 Necrosis of skin and deeper tissues can occur rapidly, and there is a very high mortality unless the diagnosis is made promptly and radical management undertaken. Preceding surgery and instrumentation in patients with the listed risk factors is particularly important.
In adults the mortality is approximately 25%, but it is lower in children.3,5
The clinical differential diagnosis of Fournier gangrene includes trauma, herpes simplex, cellulitis (streptococcal, staphylococcal), streptococcal necrotizing fasciitis, gonococcal balanitis and edema, ecthyma gangrenosum, allergic vasculitis, polyarteritis nodosa, necrolytic migratory erythema, vascular occlusion syndromes, and warfarin necrosis.
A
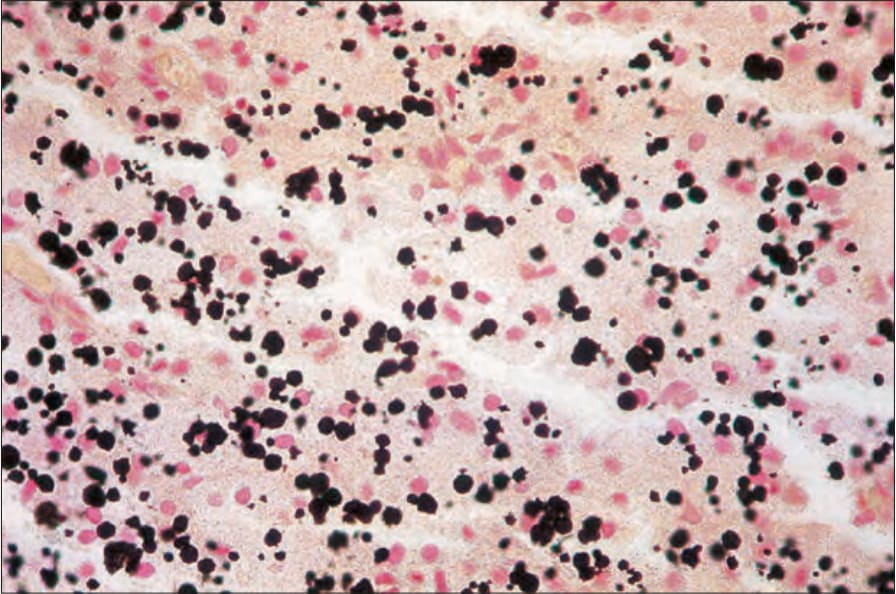
Fig. 12.147 Malacoplakia: the Michaelis-Gutmann bodies can be highlighted with the von Kossa reaction.
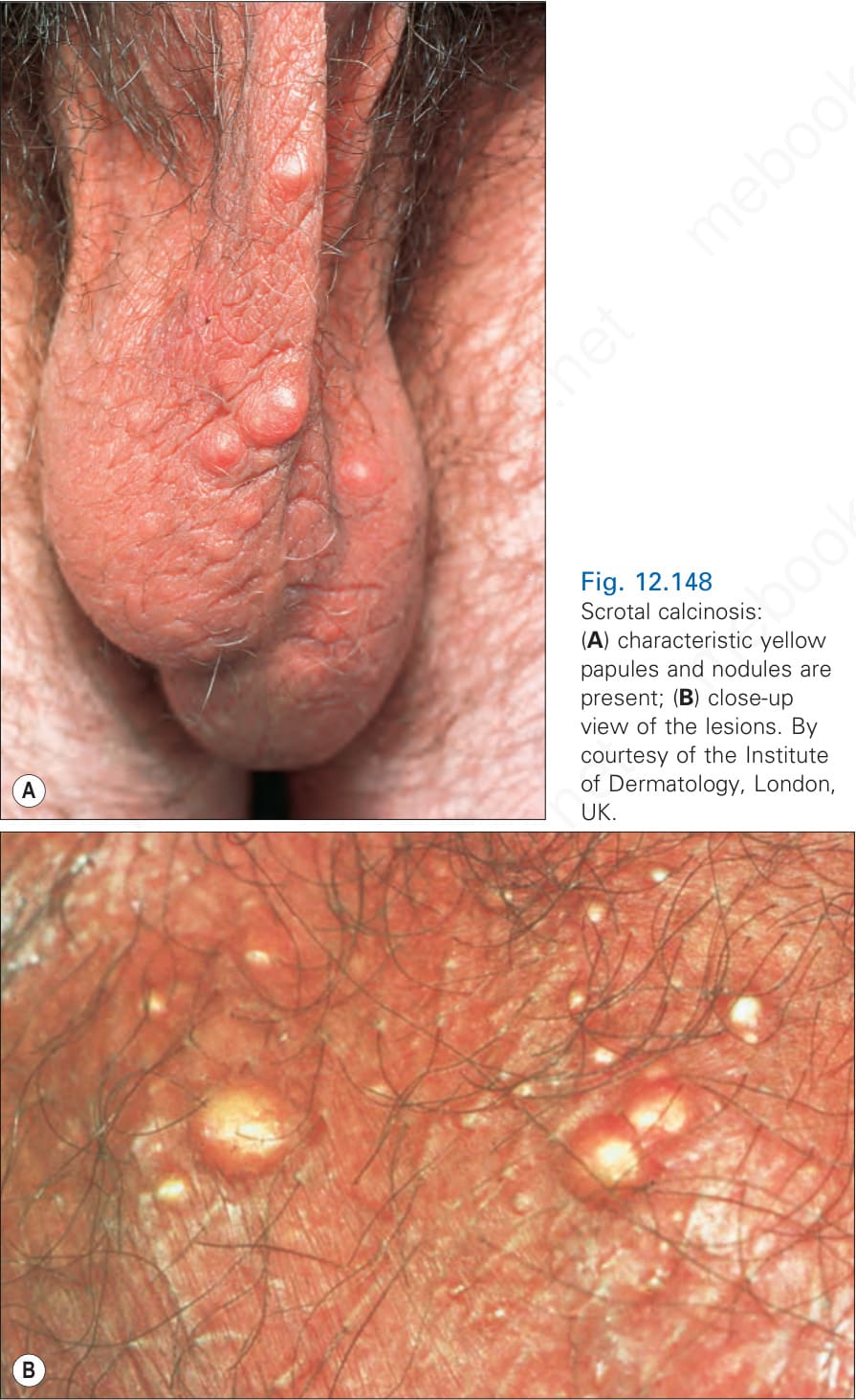
Fig. 12.148 Scrotal calcinosis: (A) characteristic yellow papules and nodules are present; (B) close-up view of the lesions. By courtesy of the Institute of Dermatology, London, UK.