Malacoplakia
Malacoplakia
Clinical features Malacoplakia (soft plaque) is a result of impaired macrophage function in the inflammatory response to bacterial pathogens, most notably Escherichia
513 Infectious diseases
coli, but other organisms, including S. aureus, Proteus, Pseudomonas, Klebsiella, and mycobacteria, can be involved. Primary or acquired immunodeficiency has been found in 40% patients.1 The latter include HIV and solid organ transplantation, mainly renal, and very rarely, heart transplant.2,3
It is most frequently described affecting the urinary tract, but it can involve many other organs including the gastrointestinal system, lymph nodes, lower genital tract, brain, bone, lungs, adrenals, and skin.4,5 Cutaneous lesions may be dermal and/or subcutaneous and are most common around the genitalia (particularly the vulva) or perineum in about 41% of cases, but can be seen at other sites including the trunk in 20% of patients, head and neck in 20%, limbs in 10%, and axilla in 10%.5 Involvement of Bartholin gland has also rarely been reported.6 Vaginal bleeding may occur. Concomitant infection with granuloma inguinale of the cervix is described in one patient.7 Multiple cutaneous sites can be involved, and in an exceptional case there was involvement of the skin with extension into the calvarium and the brain parenchyma.5 Cutaneous manifestations are variable and include papules, plaques, polyps, ulcers, and sinuses.
Underlying or related conditions, which are usually associated with immunosuppression, include carcinoma, rheumatoid arthritis, systemic lupus erythematosus, hepatitis C, sarcoidosis, leukemia, lymphoma, and transplantation. The skin lesions are nonprogressive, but are typically persistent.
Pathogenesis and histologic features Malacoplakia is characterized by confluent sheets of histiocytes with eosinophilic granular cytoplasm and small, usually eccentric, nuclei. There are characteristic cytoplasmic, calcified, von Kossa-positive inclusions known as Michaelis-Gutmann bodies (Figs 12.146 and 12.147). These are sometimes laminated, and this can be accentuated with PAS staining. They may also be positive on staining with Perl’s reaction for iron. The Michaelis-Gutmann body is sufficiently distinctive to allow cytological distinction of malacoplakia in a preparation from a skin scraping.8,9 The histiocytic infiltrate may be mixed with neutrophils, lymphocytes, and plasma cells, with associated granulation tissue. Electron microscopy of malacoplakia shows the histiocytes to contain numerous phagolysosomes, sometimes with intact and/or partly digested bacteria. It appears that the phagolysosomes accumulate in response to chronic bacterial infections.
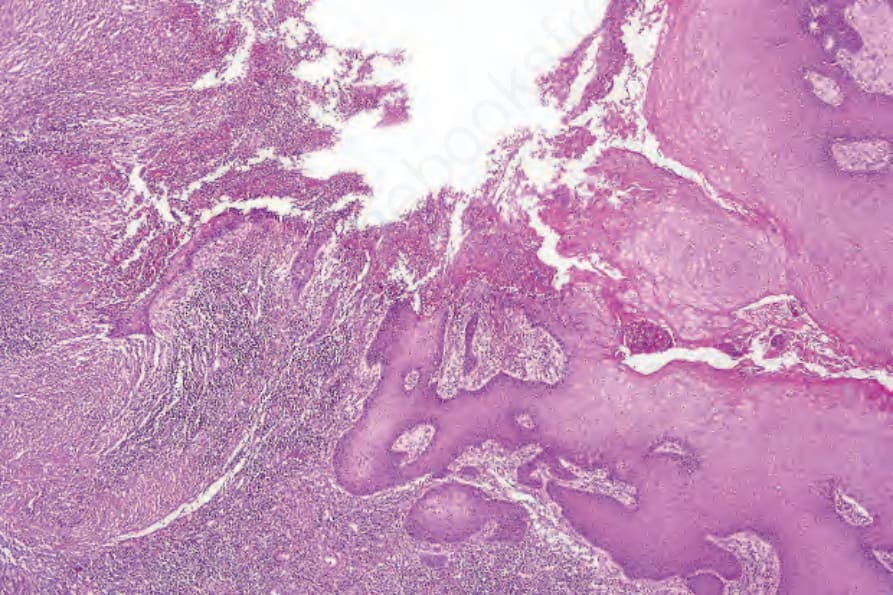
Fig. 12.143 Amebiasis: biopsy from a vulval ulcer, which developed as a result of direct spread from the anus.
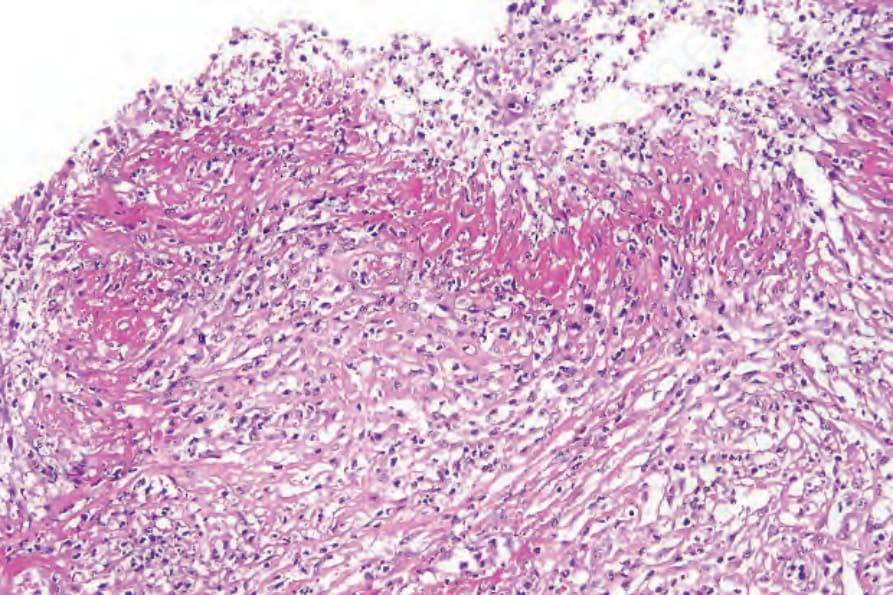
Fig. 12.144 Amebiasis: the floor of the ulcer is covered by a dense fibrinous exudate.
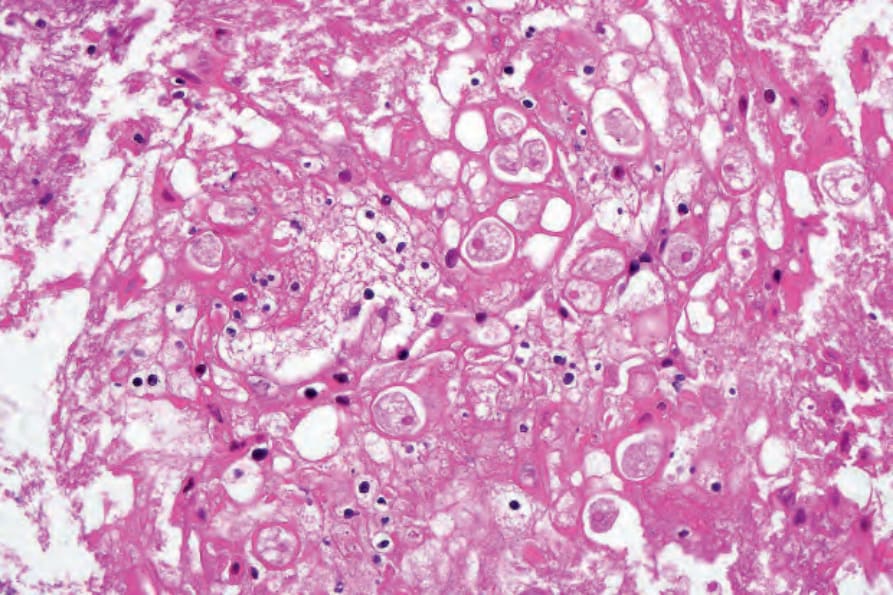
Fig. 12.145 Amebiasis: there are numerous trophozoites present. Note the ingested red blood cells.
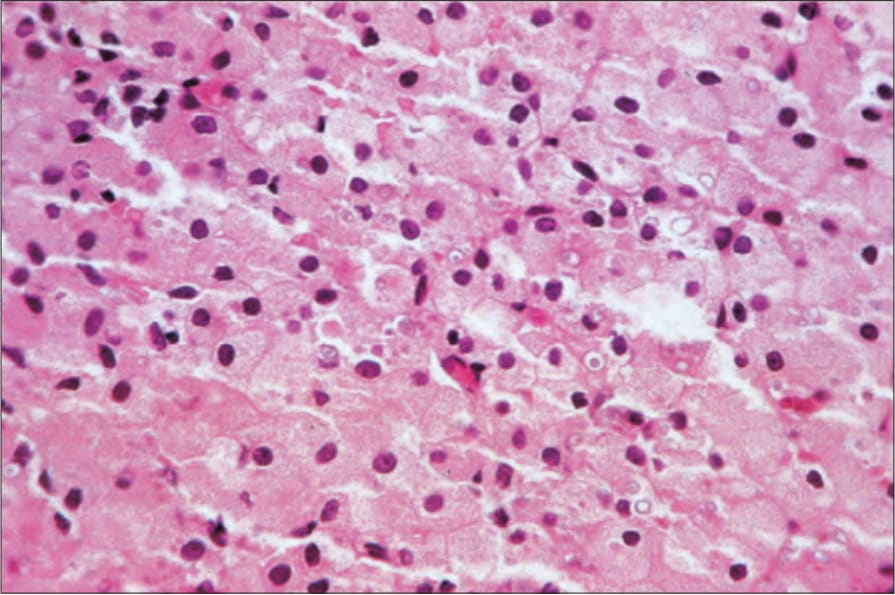
Fig. 12.146 Malacoplakia: the infiltrate consists of histiocytes with eosinophilic cytoplasm. Note the pale blue, laminated Michaelis-Gutmann bodies.