Schistosomiasis
Schistosomiasis
Clinical features Schistosoma hematobium and Schistosoma mansoni are both found extensively in Africa. S. mansoni also occurs in the West Indies and in parts of South America. Schistosoma japonicum is present in China, Japan, and Southeast Asia. These trematodes (blood flukes) do not often cause major disease of the skin, but skin lesions do occur at various stages of infestation.1
511 Infectious diseases
Invasion of the human host by the aquate cercarial stage may be associated with dermatitis (swimmer’s itch). This rash is erythematous, pruritic, and urticarial, but eventually resolves to leave a pigmented spot. It is more often encountered with invasion of avian species.
In schistosomiasis (bilharziasis), the mature worms may be associated non-specifically with erythematous itching macules at the time of release of large numbers of eggs. This probably represents a systemic reaction to antigen liberation. A more severe reaction seen particularly with S. japonicum is Katayama disease or Yellow River fever. In addition to erythema, macules, and pruriginous lesions, patients may also have fever, malaise, chills, sweats, arthralgias, headache, lymphadenopathy, hepatosplenomegaly, and peripheral blood eosinophilia.2
Specific skin lesions are seen, usually around the genitalia and most often in prepubertal females, when ova are deposited there (Fig. 12.137). They appear as grouped solid papules, which subsequently become warty and vegetative, resembling condyloma acuminatum (Fig. 12.138). The labia majora are often involved initially. Occasionally, progression to SCC occurs. Periurethral granulomata due to schistosomes may be associated with thrombosis and necrosis, sometimes resulting in fistula formation in the perineum (‘watering can perineum’). In late lesions prominent scarring may occur. More rarely, entrapped ova are seen in other areas of skin, but the means of their migration to those sites is not understood. Extragenital lesions of schistosomiasis have been described in the trunk (mainly periumbilical but also in the axilla, back and inframammary area), face, and proximal lower limbs.3 Facial lesions may be associated with ocular involvement.4 Extragenital schistosomiasis, also known as extragenital bilharziasis cutanea tarda, is very rare and its recognition is extremely important as it is usually a sentinel as well as a potential external marker of recurrent visceral disease. Interestingly, it has been noted that this type of disease often occurs in preexisting cutaneous pathology such as squamous papilloma, SCC, scarring, and hidradenitis suppurativa.3
sequelae are a direct consequence of the immunological response to their presence.
Eggs are released into the urine or feces where they hatch, releasing miracidia, which enter the snail host. Involvement of the female genital tract is usually due to S. hematobium and occurs as a consequence of worms being transported via anastomoses between the vesical and uterovaginal venous plexuses.
Pathogenesis and histologic features Part of the life cycle of schistosomes takes place in water snails. After their release from the snails, the cercaria penetrates the skin of humans and migrate as schistosomes to the portal veins where they mature into adult male and female worms. Adult females then migrate to the mesenteric plexus (S. mansoni and S. japonicum) or vesical plexus (Schistosoma haematobium). Ova are deposited in the venules, and the clinical and pathological
Histologically, adult worms are occasionally seen within the lumina of dilated deep dermal veins and lymphatics (Fig. 12.139). Viable ova may be present with a recognizable miracidial structure (Fig. 12.140). These are usually located within abscesses containing numerous neutrophils and variable numbers of eosinophils. Poorly formed granulomata with Langhans giant cells are also sometimes a feature. S. hematobium is recognized by its terminal spine (Fig. 12.141). S. mansoni has a lateral spine and S. japonicum has no spine. The dead ova typically calcify and provoke a chronic, frequently granulomatous, inflammatory response. The overlying epidermis is usually acanthotic, sometimes to the point of pseudoepitheliomatous hyperplasia and may occasionally contain intraepidermal ova undergoing transepidermal elimination (Fig. 12.142).5,6 Smearing crushed biopsies between two
512 Diseases of the anogenital skin
suspected.3 Cutaneous lesions have been recorded on the trunk, buttocks, face (including the eyelid and the orbit), genitalia, perineum, and on the legs.4,5 The cervix is often affected in genital lesions. Subcutaneous swellings called amebomas have been described. Patients with deep tissue involvement tend to have associated contiguous disease, and the prognosis tends to be worse. In HIV/AIDS the outcome is associated with coexisting systemic diseases, and death may ensue in patients with extensive internal involvement.6
Lesions present as cutaneous ulcers with a central necrotic zone covered by a purulent exudate, an undermined margin and an erythematous halo. The ulcers are irregular, but sharply defined. They spread and do not heal spontaneously. They are extremely painful and may be destructive. Presentation can also be with fistulae, fissures, abscesses, and polypoid or warty lesions. Occasionally, the latter are large and resemble ulcerating tumors. Sometimes they mimic SCC.7 Cases of amebiasis presenting as balanitis have been described.8 Although painful swelling and ulceration are the principal clinical features, frequency, dysuria, and retention may be complications
Histologic features Lesions are characterized by prominent ulceration, necrosis, and a mixed inflammatory cell infiltrate composed of lymphocytes, histiocytes, plasma cells, and neutrophils. The trophozoites of E. histolytica are found within the purulent ulcer exudate and are best identified with PAS staining (Figs 12.143–12.145).9 They are distinguished by their tendency to phagocytose red blood cells. Trophozoites and cysts are usually found in the patient’s feces. The organisms are surrounded by neutrophils, with some lymphocytes and plasma cells. The adjacent epidermis appears acanthotic, and this may be marked or pseudoepitheliomatous in verrucous forms. In some cases there is thrombosis or vasculitis with intravascular amebic trophozoites.
glass slides with 0.5% trypan blue in saline helps to highlight the ova.7 Adult parasites can sometimes be identified in anogenital and extragenital lesions.3
Identification of the type of schistosoma can be made by molecular methods.8

Fig. 12.137 Schistosomiasis: early lesion showing labial erythema and swelling. These features are a response to ova deposition. By courtesy of P. Dowd, MD, Middlesex Hospital, London, UK.

Fig. 12.138 Schistosomiasis: this warty pale nodule has almost completely replaced the left labium majus; other vulval manifestations include schistosomal condylomata, ulcers, and rarely, vitiligo. By courtesy of the late M.S.R. Hutt, MD, St Thomas’ Hospital, London, UK.
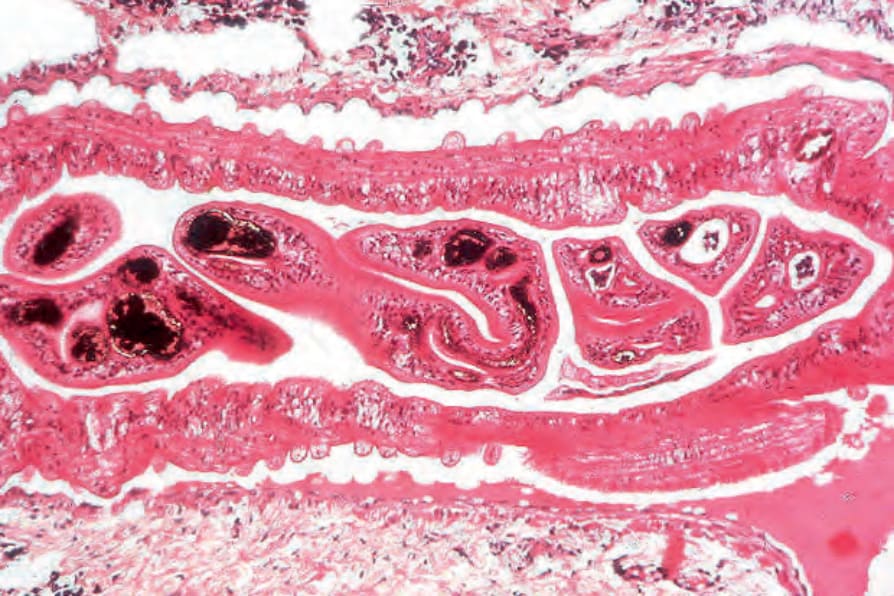
Fig. 12.139 Vulval schistosomiasis: adult worms within a dilated lymphatic; the male characteristically embraces the female in the gynecophoric canal.
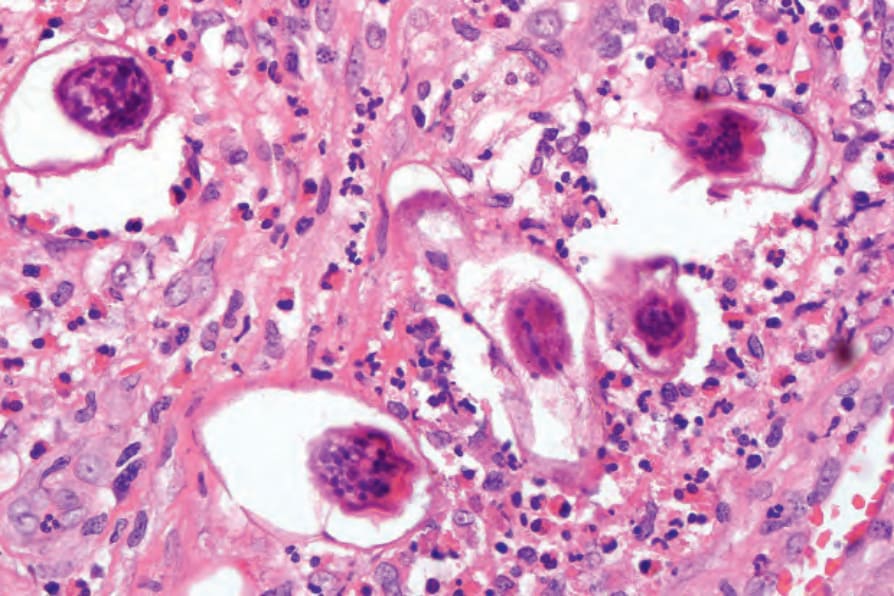
Fig. 12.140 Schistosomiasis: these ova are surrounded by a heavy infiltrate with conspicuous eosinophils.
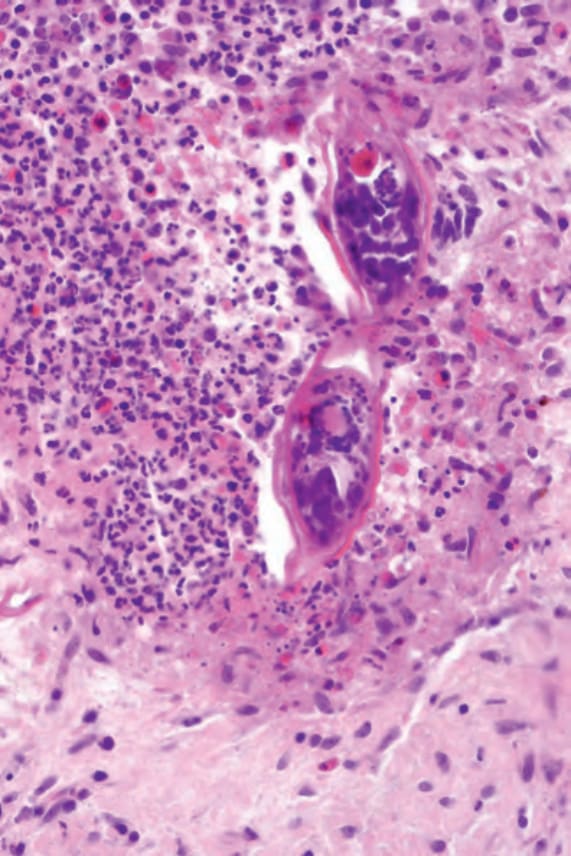
Fig. 12.141 Schistosoma hematobium: the terminal spine is characteristic of this species.
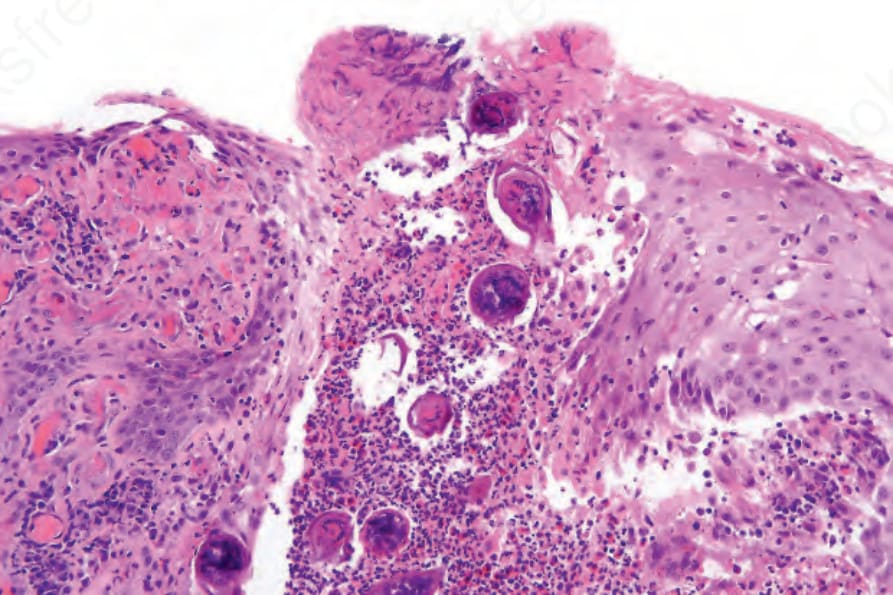
Fig. 12.142 Schistosomiasis: there is marked acanthosis. Ova are present within a breach in the epidermis.
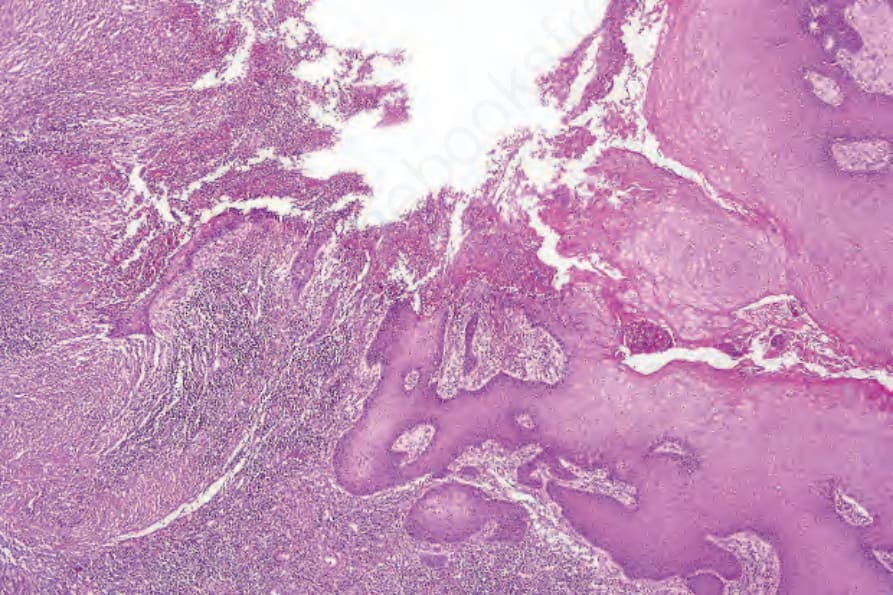
Fig. 12.143 Amebiasis: biopsy from a vulval ulcer, which developed as a result of direct spread from the anus.