Chancroid
Chancroid
Clinical features Chancroid (soft chancre, genital ulcer disease) is very common in some tropical areas of Africa, Southeast Asia, Central America, and the Pacific.1 Poor hygiene is a feature of communities where the disease is endemic. It is associated with an increased risk of transmission or acquisition of HIV.2 Genital ulcers including chancroid appear to develop more commonly in
509 Infectious diseases
HIV-positive women during the first month of antiretroviral therapy.3 It has also been diagnosed more frequently in Western Europe and North America in association with increased travel, immigration and prostitution. Chancroid was endemic in New York City and southern Florida in the 1980s. It represented 3% of genital ulcers in a sexually transmitted disease clinic in Paris.4 The disease is acquired almost always by sexual contact and has a short incubation period of 3 days to 2 weeks (median, 7 days). Exceptionally, nonsexually transmitted lower limb chancroid ulcers have been reported in patients from Papua New Guinea and Samoa, in both adults and children.5,6 Concurrence with other sexually transmitted disease including gonorrhea can be seen.7
The initial lesion is usually a transient vesicular tender papule, which rapidly ulcerates with copious suppuration. The ulcer is sharply circumscribed with an undermined edge and is typically not indurated. These lesions appear much more commonly in the male, usually on the penis (Fig. 12.132). The prepuce, coronal sulcus, frenulum, and glans are the most favored sites. Circumcised males are at lower risk of developing the disease.8 Lesions in the female are seen on the fourchette, labia majora and minora, and around the clitoris. The perineum and perianal area may also be affected. Multiple ulcers can be present, which have an irregular ragged edge and slough-covered bases. Cervical and vaginal involvement is uncommon. Variants of primary chancroid ulcers include giant and serpiginous forms, follicular, transient, and dwarf lesions; occasionally, a condyloma lata-like presentation may occur.
A
The ulcers are tender and especially painful when in contact with urine. Lymphadenitis occurs in about 50% of cases approximately 1 week after the genital lesion, and in 50% of these, suppuration (bubo formation) usually follows. Sometimes rupture may occur, resulting in inguinal ulceration. In other cases, the course is variable, some resolving without treatment in a few days while others go on for several weeks, developing phimosis or even gangrene. Systemic infections do not occur.
B
Pathogenesis and histologic features Chancroid is caused by Haemophilus ducreyi, a Gram-negative coccobacillus, which grows in chains sometimes arranged in parallel. It is transmitted through minor abrasions during sexual intercourse. The subsequent lesion comprises:
• a superficial zone of neutrophils, red cells, bacteria, and cell debris,
• a middle zone of edematous granulation tissue,
• an underlying infiltrate of histiocytes, lymphocytes, and plasma cells (Figs 12.133 and 12.134). The enlarged lymph nodes show central necrosis with a surrounding mixed inflammatory response of neutrophils and macrophages.
510 Diseases of the anogenital skin
Diagnosis is confirmed by isolation of the organism by culture in a blood-enriched medium containing vancomycin at 33°C. The bacterium may be identified by its chain-like growth in scrapings from the margin of the ulcer, but secondary organisms are often present and it is more helpful to identify the organism in an aspirate from a necrotic lymph node. DNA in situ hybridization and PCR for H. ducreyi has been developed.9,10 DNA from the organism has been detected by PCR in esophageal lesions of HIV-positive patients.11
or rectal primary lesion may be complicated by a stricture of the rectum 5–10 cm from the anus.7 This is associated with periproctitis and proctocolitis, which sometimes fistulates.8 Rectal carcinoma is an occasional late complication.9 In both sexes, genital lymphedema and even elephantiasis can develop after the lymphadenopathy. This may be a continuing problem and can be associated with secondary cutaneous erosions and ulceration. Systemic lesions are rare, and include cardiac and pulmonary involvement, keratoconjunctivitis, episcleritis, uveitis, papilledema and retinal hemorrhages, meningitis, hepatitis, and cutaneous manifestations such as erythema nodosum and erythema multiforme.10
Pathogenesis and histologic features Lymphogranuloma venereum is caused by strains L1, L2, and L3 of the bacterium C. trachomatis. The C. trachomatis species is divided into 15 prototypic serovars according to analysis of their outer membrane protein.11 Only serovars L1 to L3 are associated with lymphogranuloma venereum, with the L2 serovar causing most cases. Chlamydiae are nonmobile, coccoid, obligate intracellular parasites. They depend on their host cells for ATP metabolites and multiply within membrane-bound vacuoles in the host macrophage cytoplasm. They stain faintly blue with hematoxylin and eosin (H&E), Gram-negative with the Brown-Hopps tissue Gram stain, and black with the Warthin-Starry silver impregnation technique.12 On the rare occasions that the primary lesion is viewed histologically, the base of the ulcer is lined by intensely inflamed fibrous granulation tissue. Plasma cells and microabscesses are present. The lymphadenitis has a characteristic picture of stellate central necrosis with neutrophils and a surrounding palisaded granulomatous reaction with occasional giant cells.
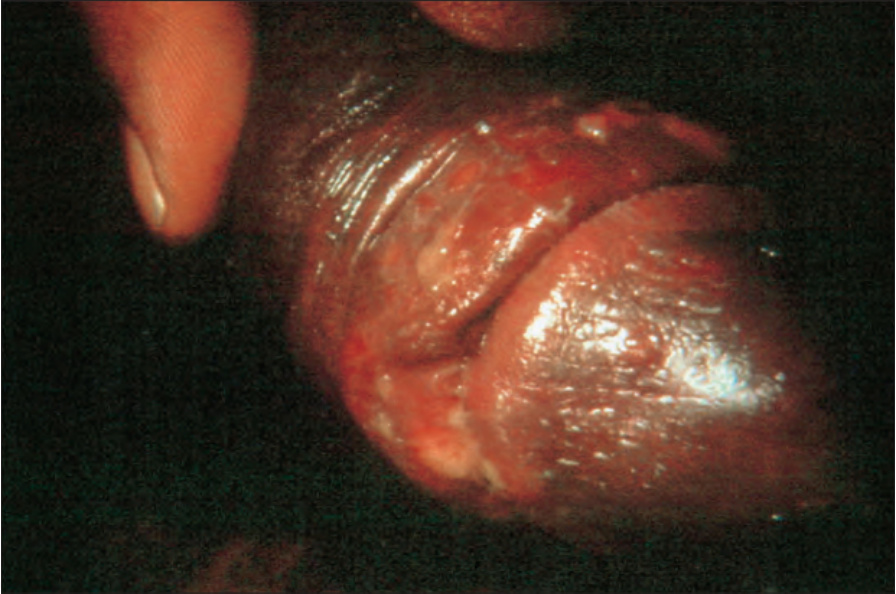
Fig. 12.132 Chancroid: irregular ulcer extending along the coronal sulcus of the penis. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.
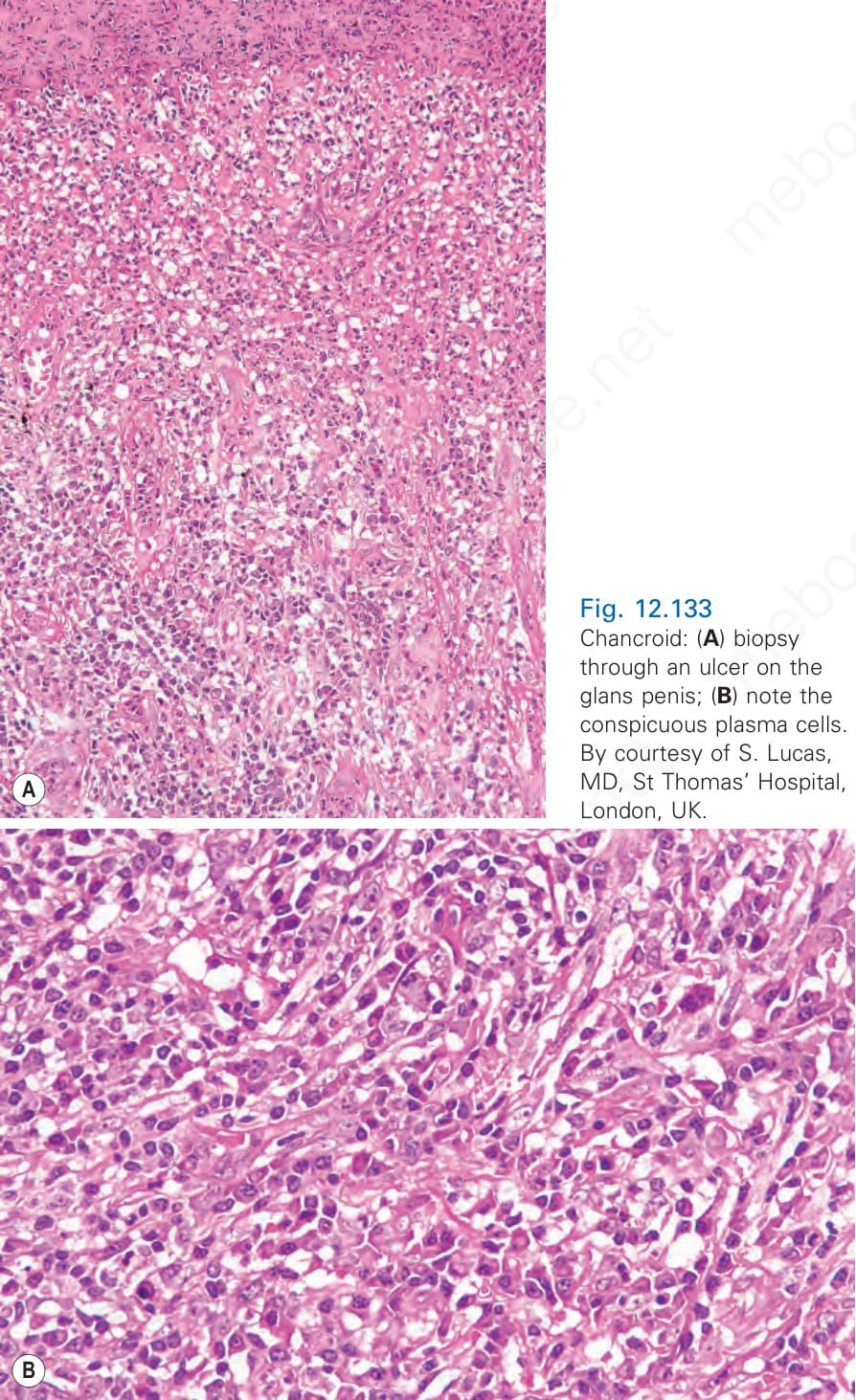
Fig. 12.133 Chancroid: (A) biopsy through an ulcer on the glans penis; (B) note the conspicuous plasma cells. By courtesy of S. Lucas, MD, St Thomas’ Hospital, London, UK.
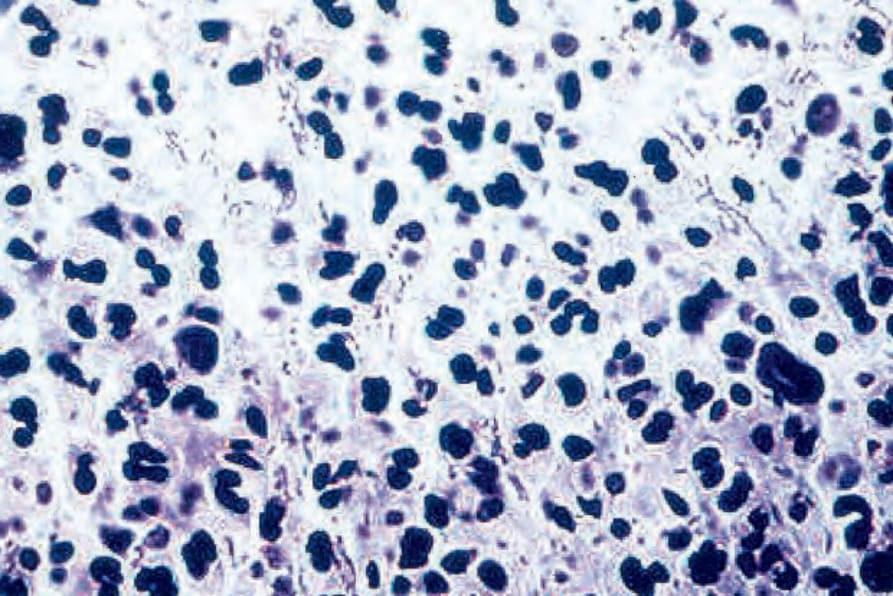
Fig. 12.134 Chancroid: note the coccobacilli growing in chains.
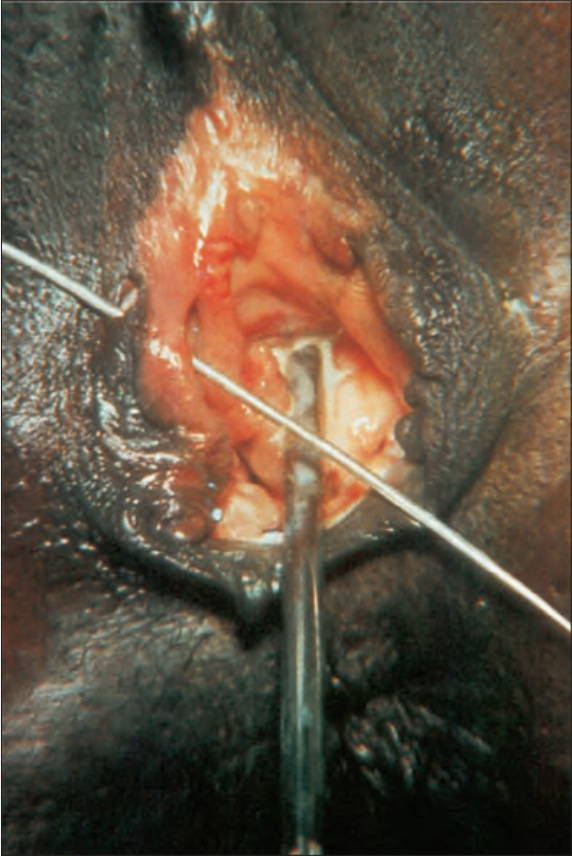
Fig. 12.135 Lymphogranuloma venereum: note the ulcer on the right labium majus. By courtesy of S. Lucas, MD, St. Thomas’ Hospital, London, UK.

Fig. 12.136 Lymphogranuloma venereum: there is an ulcer on the penile shaft covered with necrotic debris. By courtesy of the Institute of Dermatology, London, UK.