Granuloma inguinale
Granuloma inguinale
Clinical features Granuloma inguinale (donovanosis) occurs in people with poor hygiene in tropical regions, mainly in India, Brazil, the West Indies, China and West Africa; it was formerly seen in southern United States, but is now rare.1 The disease is still seen in Australia in the Aboriginal population.2 The organism is of low infectivity and is presumed to be spread by sexual contact, probably through abraded skin. It occurs most often in the third to fifth decades. The incubation period is uncertain and may range from 2 to 3 weeks to several months.
The initial presentation in females is usually of one or more indurated papules or nodules on the inner aspect of the labia, the fourchette, or around the clitoris (Fig. 12.127).3 In males, the glans, prepuce, coronal sulcus, or shaft is affected (Fig. 12.128). Dorsal perforation of the prepuce can occur
507 Infectious diseases
as a late complication.4 The perianal and inguinal regions and the cervix may also be involved.5–7 In one case involving the cervix, there was associated malacoplakia.7 The papules ulcerate irregularly and extend widely if untreated. The base of the ulcer is ‘beefy’, and the margins are undermined and indurated. Spread to contiguous ‘kissing’ areas may sometimes occur. Variants include verrucous, necrotic, and scarring lesions. Primary infection of the lymph nodes does not occur, but painful lymphadenopathy is common due to secondary infection. Rarely, primary extragenital lesions may be seen (mainly mouth or lips but also at unusual sites such as the foot).8,9 Exceptionally, presentation as a psoas abscess and as a pelvic mass mimicking ovarian cancer has been described.10,11
Very occasionally, there is a systemic infection with involvement of many organs including the liver, and osteolytic lesions in bone.12 The latter may particularly relate to a primary cervical lesion.1 Spinal compression has also been reported.13 Later complications include strictures of the urethra, vagina, or anus, destruction of the penile shaft with autoamputation, and pseudoelephantiasis.14–17 As with other sexually transmitted diseases, patients
508 Diseases of the anogenital skin
with granuloma inguinale are often HIV positive and may also have syphilis.18 Genital SCC is an uncommon but important complication.19,20 Infection in children has rarely been reported and occurs as a result of transmission from an infected mother at birth.21 Rare manifestations of the disease in children include a mass in the neck, otitis media, and mastoiditis.22,23
is associated acanthosis, which sometimes amounts to pseudoepitheliomatous hyperplasia. Ulceration is common. A large study has demonstrated frequent transepidermal elimination of organisms.25 It is likely that this phenomenon may be an important mechanism in the spread of the disease.
Pathogenesis and histologic features Granuloma inguinale is caused by Calymmatobacterium granulomatis (formerly Donovania granulomatis), an encapsulated short (1–2 µm) Gram-negative rod with characteristic bipolar staining. It is transmitted by sexual contact, but it is of low infectivity.1 The organism is found in feces, and this may act as a reservoir of infectivity or, in occasional cases, be the source of genital infection. The higher incidence of infection in homosexuals may support this concept.
The lesion is characterized by a very intense inflammatory infiltrate in which plasma cells are predominant (Fig. 12.129). Focal formation of neutrophilic microabscesses is frequent. Pathognomonic macrophages contain cytoplasmic cyst-like vacuoles in which bacteria can be demonstrated by staining with Giemsa or the Warthin-Starry reaction (Figs 12.130 and 12.131).24 The bacteria can also be seen extracellularly. In most cases there
Diagnosis is confirmed by the identification of typical organisms (Donovan bodies) on a scraping from an ulcer or in a biopsy stained with Giemsa or Warthin-Starry. PCR has also been used successfully to confirm the diagnosis.26 Dark-field illumination microscopy should be performed to exclude syphilis. By electron microscopy, the encapsulated microorganisms can be demonstrated within the phagosomes of macrophages.27
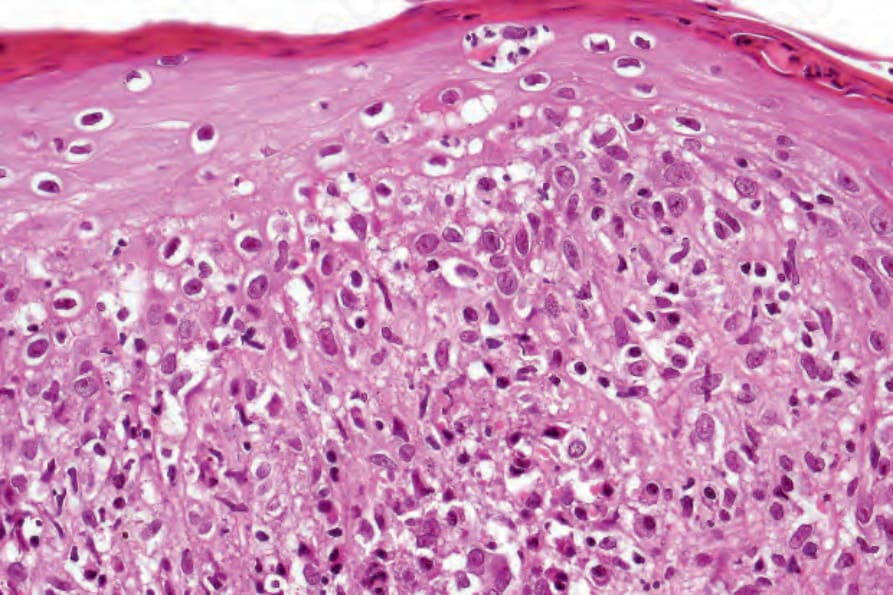
Fig. 12.122 Secondary syphilis: in this field, there is marked interface change.
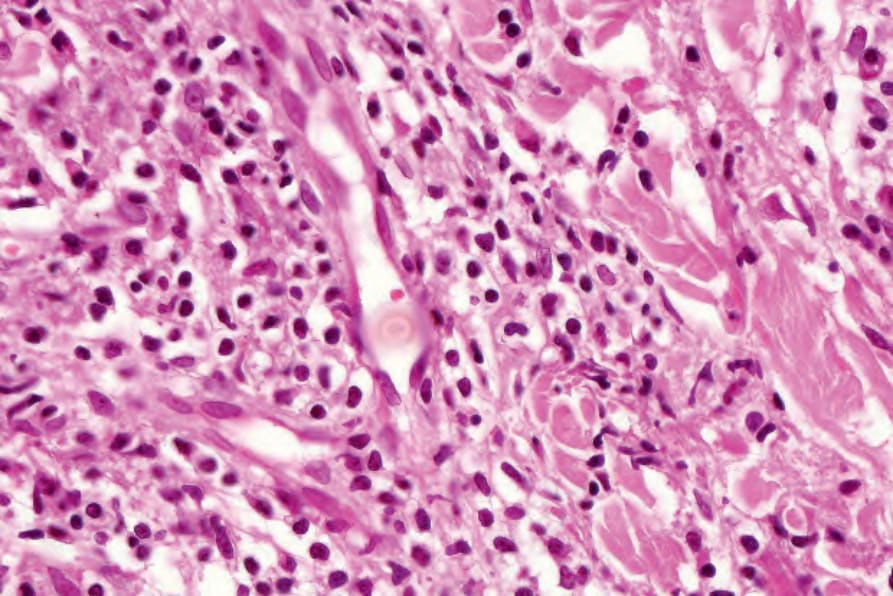
Fig. 12.123 Secondary syphilis: note the marked endothelial cell swelling.
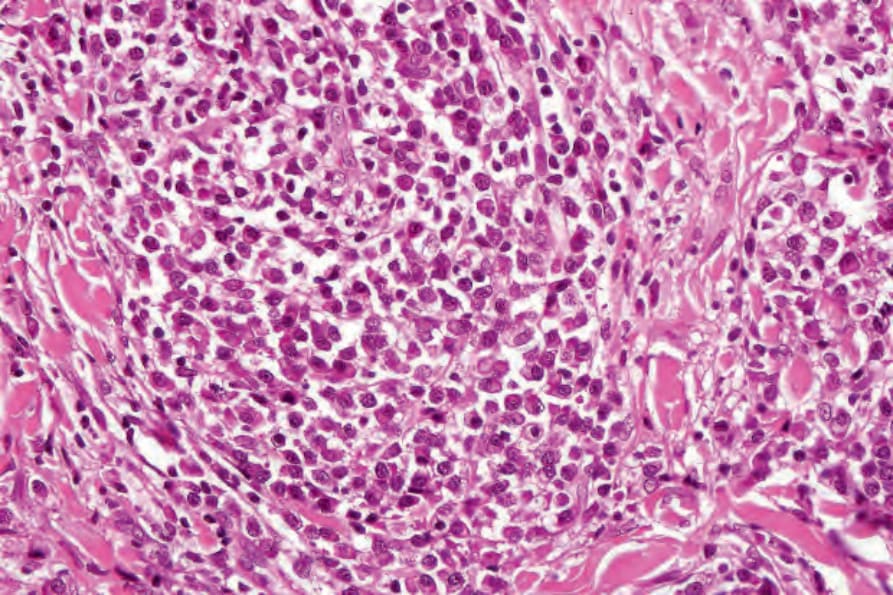
Fig. 12.124 Secondary syphilis: innumerable plasma cells are present.
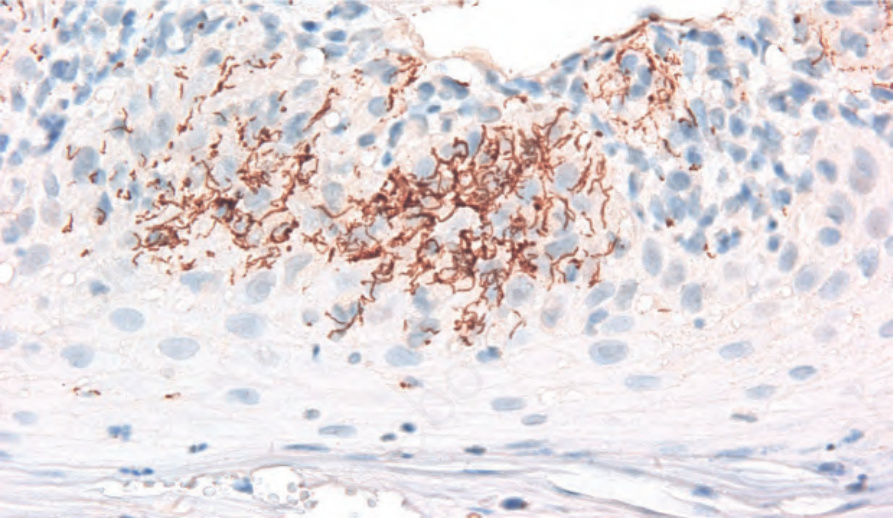
Fig. 12.125 Secondary syphilis: numerous spirochetes are seen by immunohistochemistry within the epidermis in a patient with secondary syphilis.
Fig. 12.126 Gumma: high-power view reveals ghost outlines of cells and connective tissue.

Fig. 12.127 Granuloma inguinale: early lesion showing an ulcerated papule adjacent to the clitoris. By courtesy of J. Lawson, MD, University of Newcastleupon-Tyne, UK.

Fig. 12.128 Granuloma inguinale: in this patient, there is extensive ulceration of the glans penis. Note the typical ‘beefy’ appearance. By courtesy of C. Furlonge, MD, Port of Spain, Trinidad.
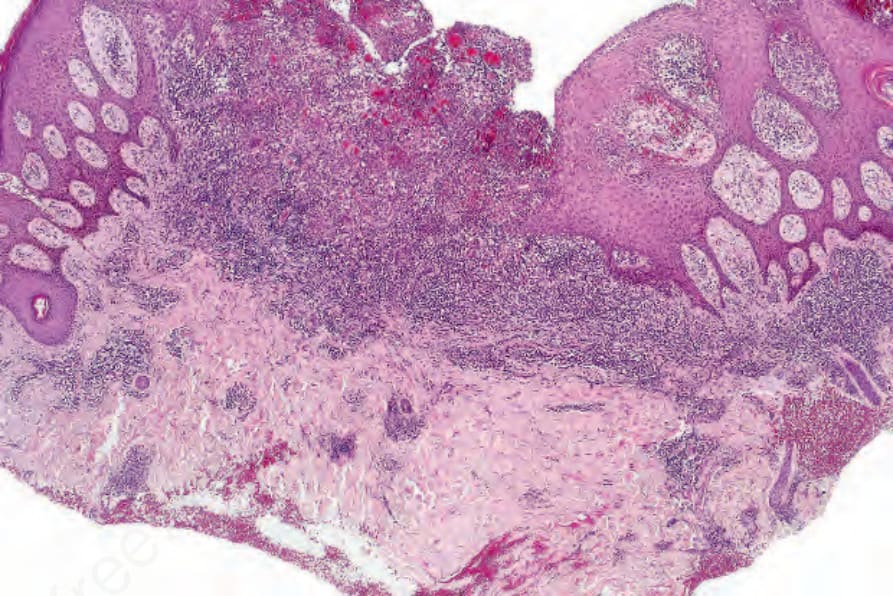
Fig. 12.129 Granuloma inguinale: biopsy from the penis. Note the pseudoepitheliomatous hyperplasia. There are intense inflammatory changes.
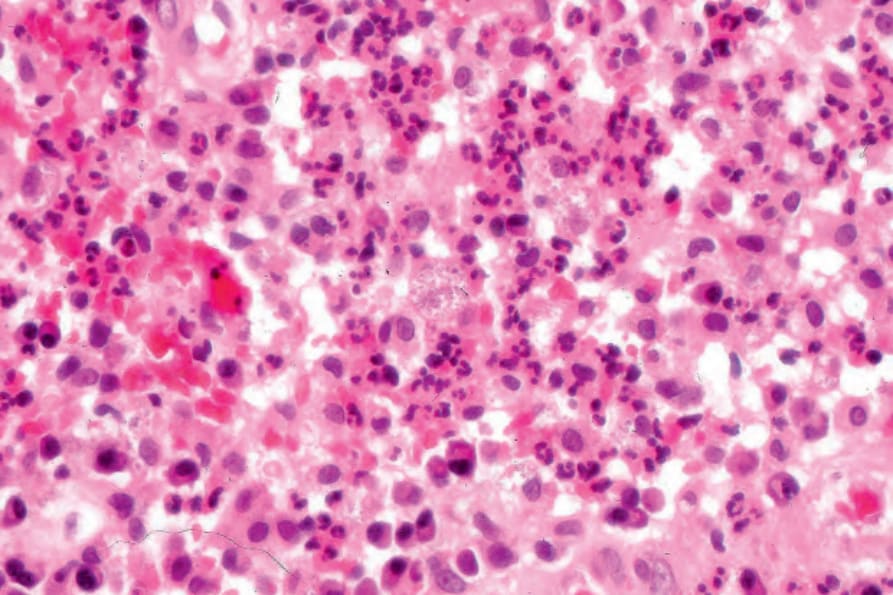
Fig. 12.130 Granuloma inguinale: the infiltrate consists of lymphocytes, neutrophils, plasma cells, and conspicuous pale-staining histiocytes.
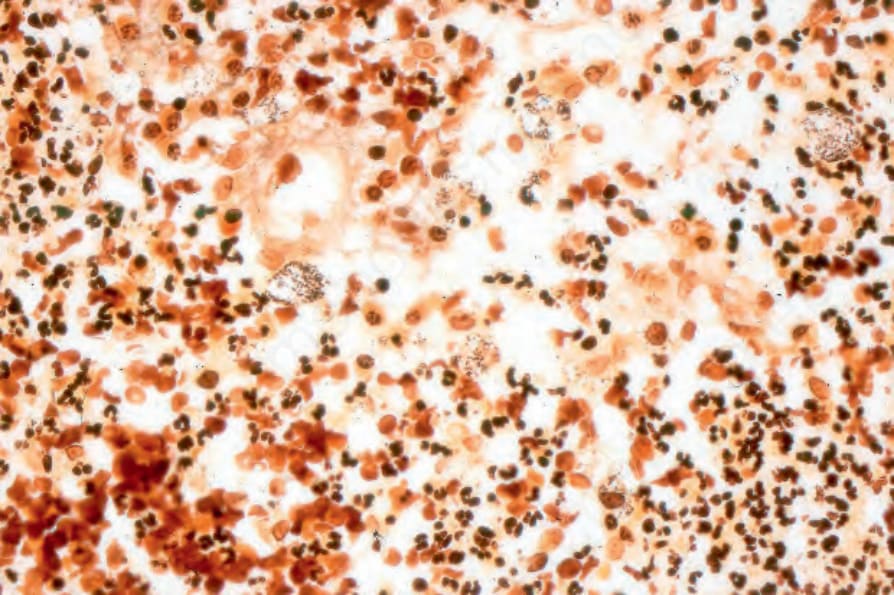
Fig. 12.131 Granuloma inguinale: the histiocytes contain characteristic Donovan bodies (Warthin-Starry stain).