Condyloma acuminatum (genital warts, HPV infection)
Condyloma acuminatum (genital warts, HPV infection)
Clinical features Genital warts (condyloma acuminatum) are usually caused by HPV types 6, 11, 16, 18, 30–32, 42–44, and 51–55.1 HPV-7, usually associated with warts in butchers, can exceptionally be the cause of condylomas.2 HPV-6 and 11 account for approximately 90% of these lesions.3 However, more than one HPV type can be isolated from a single lesion.4 They occur on the glans penis and prepuce or shaft as soft, fleshy (sometimes filiform) plaques and may extend into the meatus (Figs 12.86 and 12.87). On the shaft, they are less exophytic. Vulval lesions may be bulky and macerated, and can extend
into the introitus (Figs 12.88–12.90). Lesions may be difficult to detect on clinical examination.1 Vulval condylomata usually involve the labia minora, interlabial sulcus, or the area around the introitus. Similar fleshy and filiform soft masses may occur perianally and in the anus, more often in males (Fig. 12.91). Genital warts in children always raise the possibility of sexual abuse but can occur with close nonsexual contact.5 However, nonvenereal viral warts (verruca vulgaris) mainly caused by HPV type 2 can occur in both young girls and less frequently in adult women, so HPV typing can be very important.6 Young sexually active adults are the most frequently affected (second and third decades), and often in association with other sexually acquired infections.
498 Diseases of the anogenital skin
A
B
Rarely, condyloma acuminatum presents in the oral cavity.7 Condylomata have also been reported in the abdominal pannus fold of a few obese patients.8
It is important to recognize that a significant proportion of genital HPV infections are asymptomatic.1 The female partners of male patients with genital warts have been shown to have an increased risk of cervical HPV infection and intraepithelial neoplasia.9 Cervical neoplasia associated with preexistent vulval warts has also been related to immunosuppression, at least in some patients.10 Up to 80% of invasive cervical squamous carcinomas have been shown to contain HPV DNA. Types 16, 18, 31–33, 35, 39, 42, and 51–54 are most commonly associated with cancer of the cervix,
499 Infectious diseases
Histologic features Condylomata acuminata are characterized by marked acanthosis with a solid or trabecular pattern and a broad, rounded, exophytic growth (Figs 12.92 and 12.93). There is a sharp, fairly regular, deep margin. The surface of the lesion is hyperkeratotic and parakeratotic. Superficial vacuolated keratinocytes (koilocytes) are characteristic (Fig. 12.94). The vacuolated epithelium is often most marked in the declivities. Care must be taken not to confuse koilocytes with the vacuolated, glycogenated keratinocytes of mucosal epithelia or with artifactually vacuolated keratinocytes. Distinction can be made fairly readily as koilocytes have an enlarged, wrinkled, hyperchromatic nucleus.
vulva, and penis11,12 Malignant transformation of genital warts is rare but may be found in association with penile bowenoid papulosis and VIN usual type (undifferentiated).11,13 In the most recent classification of VIN,14 condylomata acuminata are classified as low-grade squamous intraepithelial lesions.14
A large, exuberant, and locally destructive variant of condyloma (Buschke-Löwenstein tumor) may rarely be encountered.15 This is associated with HPV-6, 11, or 16. It is considered by many to be a variant of verrucous carcinoma, a subtype of well-differentiated squamous carcinoma (see below). However, the issue remains controversial and other authors regard it as a distinctive entity. They may show malignant progression if irradiated. The condition has been described in an HIV-positive patient.16
Juvenile laryngeal papillomata containing HPV-6 and 11 can be seen in children born to mothers with condylomata acuminata.1
Care should be taken in the histologic interpretation of lesions that have previously been treated with podophyllin (although this treatment is seldom used nowadays since the advent of imiquimod). These can display prominent degenerative changes with cytoplasmic vacuolation, nuclear enlargement, and metaphase arrest. The changes, however, tend to be more focal, and abnormal mitotic figures are not seen.17,18 Immunohistochemical stains for papillomavirus common antigen have been used to confirm the diagnosis, but this is only positive in about 60% of cases.19 More recently, broad-spectrum in situ hybridization in paraffin-embedded tissue has become available.20
500 Diseases of the anogenital skin
Giant condyloma acuminatum (Buschke-Löwenstein tumor) occurs most frequently on the genitalia, and is larger and more cauliflower-like.21 It shows some tendency to endophytic growth, but without any suggestion of frank infiltration. It can recur locally. Anal condylomata may develop bowenoid features, and occasionally invasive tumors supervene.22

Fig. 12.85 Tinea incognito: there is extensive involvement of the abdomen, groins, thighs and scrotum. This followed injudicious use of topical steroids. From Bunker C. Male Genital Skin Disease. Saunders Ltd./Elsevier 2004.

Fig. 12.86 Condyloma acuminatum: multiple erythematous, velvety plaques are present on the glans penis. By courtesy of the Institute of Dermatology, London, UK.

Fig. 12.87 Condyloma acuminatum: (A) in this patient, the lesions have a typical filiform appearance; (B) multiple condylomata are present on penis and scrotum. By courtesy of the Department of Genitourinary Medicine, St Thomas’ Hospital, London, UK.

Fig. 12.88 Condyloma acuminatum: multiple gray lesions are evident on the labia minora and around the vestibule. By courtesy of the Institute of Dermatology, London, UK.

Fig. 12.89 Condyloma acuminatum: in this patient, the condylomata are pedunculated and have extended onto the thighs. By courtesy of the Institute of Dermatology, London, UK.

Fig. 12.90 Condyloma acuminatum: there is very extensive disease. The patient is at considerable risk of developing cervical disease. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.

Fig. 12.91 Condyloma acuminatum: perianal involvement is likely to be associated with homosexual activity. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.
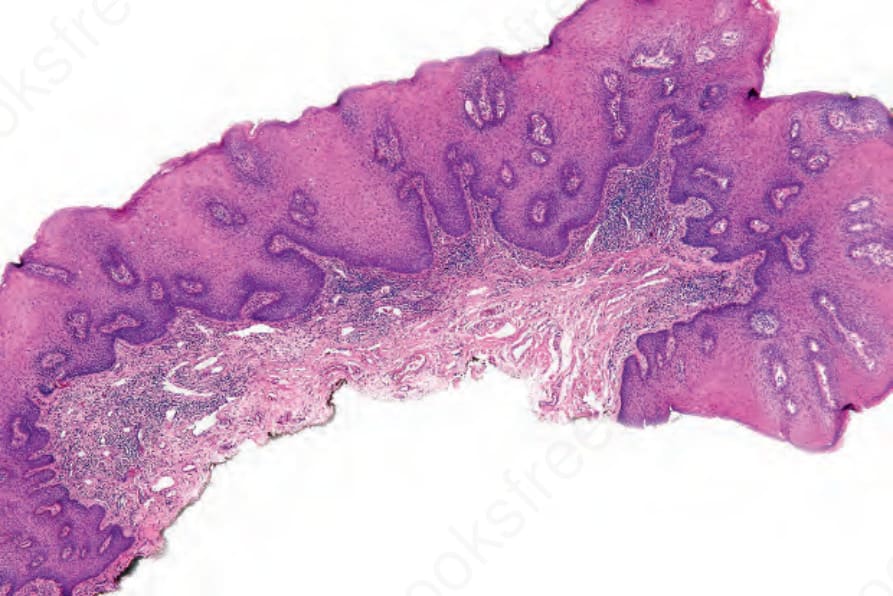
Fig. 12.92 Condyloma acuminatum: there is focal parakeratosis, slight papillomatosis and very marked acanthosis. The lower border is sharply demarcated.
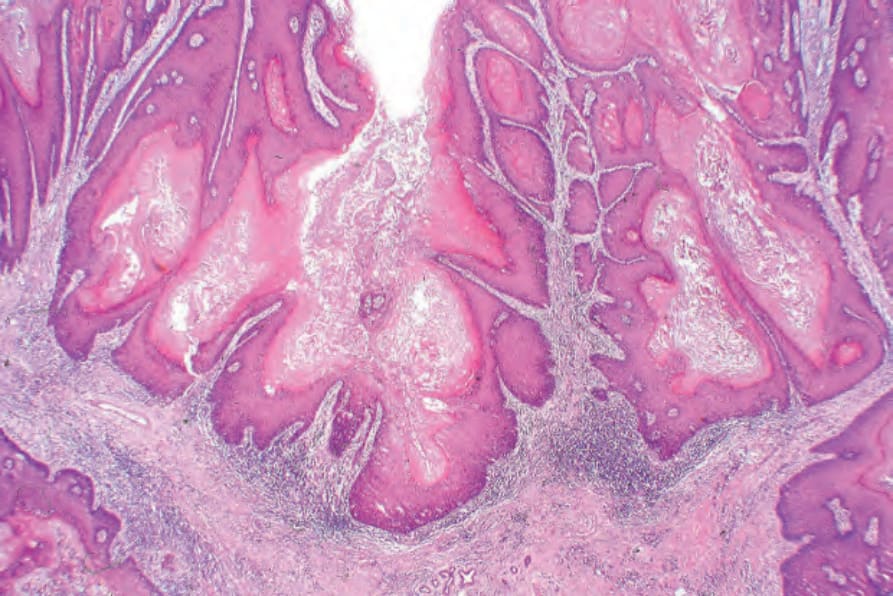
Fig. 12.93 Condyloma acuminatum: this is a much more florid example. Note the gross papillomatosis and very marked acanthosis.
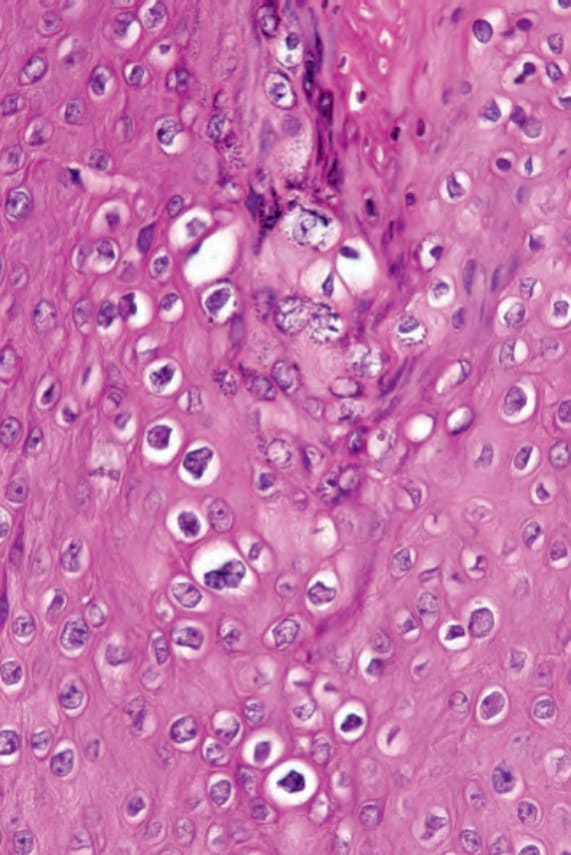
Fig. 12.94 Condyloma acuminatum: there are conspicuous koilocytes with irregular nuclei and vacuolated cytoplasm.

Fig. 12.95 Primary chancre: the chancre is a painless ulcer with an indurated edge. The base is yellow and harbors large numbers of spirochetes. By courtesy of F. Lim, MD, King’s College Hospital, London, UK.