Lichen planus
Lichen planus
Clinical features Anogenital lesions may be found in up to 40% of patients with generalized disease. In some, however, the disease is restricted to the lower genital tract and/or the perianal region. LP manifests the Koebner phenomenon which may partly explain the orogenital predilection. Genital LP in children is exceptional.1 Women with oral LP often have genital disease which may be asymptomatic.2,3
The epidermis is acanthotic with elongation and hypertrophy of the epidermal ridges and parakeratosis. The suprapapillary plates are thinned and there is infiltration of the epidermis by neutrophils, associated with vacuolation of superficial keratinocytes, together with the formation of spongiform pustules and microabscesses (Fig. 12.32). The inflammation extends into the adjacent underlying dermis, where it is predominantly mononuclear. The histology is essentially identical to that seen in pustular psoriasis.2 Therefore, close clinicopathological correlation is critical to establish a diagnosis. Occasional biopsies from typical lesions of patients with reactive arthritis may disclose an underlying leukocytoclastic vasculitis.41
A small number of patients presenting with skin lesions that histologically showed sterile neutrophilic folliculitis with perifollicular vasculopathy have been documented.42 The authors suggested that this histologic pattern may be a marker of systemic disease. Associations may include reactive arthritis, inflammatory bowel disease, Behçet disease, hepatitis B infection, scrofuloderma, connective tissue diseases, and hematological dyscrasias.
The lesions are typical, violaceous or white patches, or areas of erythema and erosions. Wickham striae (frequently seen in oral involvement), although sometimes visible, are less often found on anogenital skin (Fig. 12.33). The clinical variants of LP affecting the anogenital skin include squamo-papular, erosive, hypertrophic, and hyperpigmented flexural disease (Figs 12.34–12.41). Lichen planopilaris has also been described on the vulva.4
The erosive form of LP is more common at anogenital sites and can lead to scarring and distortion of the architecture.5 The vulval vestibule and vagina and cervix may also be involved, and sometimes the vagina and/or the cervix are affected alone.6,7 There is also an unusual variant of erosive LP in women that involves the oral gingivae, vulval vestibule, and vagina, known as the vulvovaginal-gingival syndrome (Figs 12.42–12.44).8,9 This can lead to severe vulval and vaginal scarring with vaginal adhesions, constriction bands, and, in some cases, complete stenosis.10 A male equivalent to the vulvovaginal syndrome of Hewitt with chronic erosive gingival and
483 Inflammatory dermatoses
484 Diseases of the anogenital skin
genital lesions (genito-gingival syndrome) has been described.11,12 Patients with genital lesions may have oral, aural, conjunctival, and esophageal involvement.13–17
Perianal disease can cause deep, painful fissuring, and it is often the hypertrophic variant that involves this site.
In the male genital, LP can present as phimosis.18,19 Adhesions are seen in the uncircumcised male, both transcoronal and subcoronal.
Anogenital LP carries a small increased risk of malignancy, usually squamous cell carcinoma (SCC) (Fig. 12.45).20–23 Hypertrophic LP of the glans penis should be regarded as having potential sinister biological behavior.24
485 Inflammatory dermatoses
A
Pathogenesis and histologic features Studies of oral LP have supported an immunological basis with activated T cell to an unidentified antigenic stimulus.25 The histologic features of anogenital LP are often more difficult to recognize than those of LP presenting on nonmucosal surfaces. The epidermis may be effaced or thickened, and there is a dense, band-like infiltrate hugging the dermal–epidermal junction (Fig. 12.46). Many genital lesions are mucosal and the inflammatory cell infiltrate is often rich in plasma cells, in contrast with lesions of LP at other sites where lymphocytes and histiocytes predominate (Fig. 12.47). The basal layer is often disrupted with some cytological atypia as regeneration takes place. Cytoid bodies may be seen but tend not to be prominent. This is accompanied by parakeratosis. Focal secondary spongiotic changes are not uncommon, particularly in mucosal surfaces. In long-standing disease, the dense, bandlike infiltrate may be replaced by a patchy, scant infiltrate with small foci of lichenoid inflammation. Many cases of male genital LP are misdiagnosed as ZB or LS.
B
Differential diagnosis The clinical differential diagnosis includes psoriasis, ZB in the male, LS, viral warts, bowenoid papulosis, and porokeratosis. LP is one of the causes of pruritus ani. A biopsy is frequently necessary for diagnostic purposes but is more importantly done in the follow-up of the rare cases of chronic anogenital disease where the development of ulcero-erosive or verrucous features leads to concern about the development of SCC. LP often overlaps with the features of LS, and in some patients the two disorders may coexist. Hyalinization of the papillary dermis or the superficial lamina propria is indicative of the latter condition. In patients suffering from such a chronic overlap syndrome, particular care should be taken to recognize dysplastic areas or SCC. Those patients with predominantly mucosal disease clinically mimic mucous membrane pemphigoid, but immunofluorescence studies are invariably negative. A case of paraneoplastic LP with orogenital involvement and cicatrizing conjunctivitis in association with thymoma has been described.27
Immunofluorescence studies may show fibrinogen and IgM along the basement membrane zone and, more rarely, IgG or IgA.26 Cytoid bodies may also be labeled.26
Sometimes drugs can precipitate a generalized lichenoid eruption. A case of a lichenoid drug eruption confined to the penis due to propranolol has been reported.28
486 Diseases of the anogenital skin
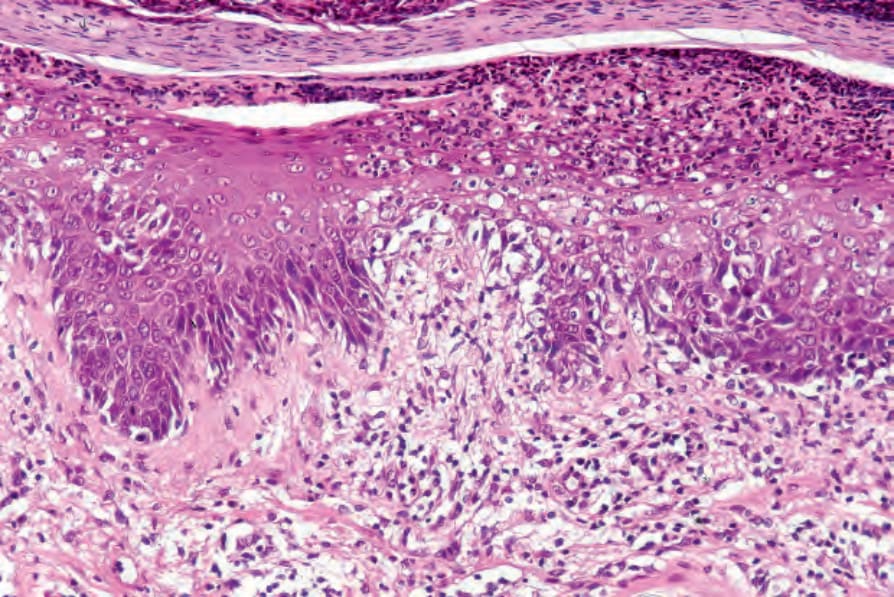
Fig. 12.32 Reactive arthritis: high-power view showing parakeratosis and a pustule.

Fig. 12.33 Lichen planus: perineal lesions showing conspicuous striae. By courtesy of the Institute of Dermatology, London, UK.

Fig. 12.34 Erosive lichen planus: there is extensive erosion of the glans penis. By courtesy of the Institute of Dermatology, London, UK.
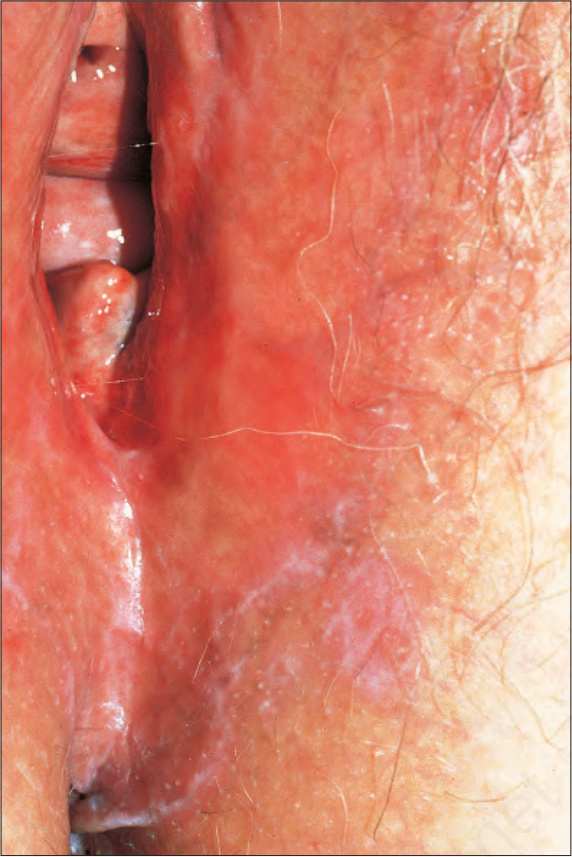
Fig. 12.35 Vulval lichen planus: reticulated lesions of lichen planus extending into the perineum. By courtesy of the Institute of Dermatology, London, UK.

Fig. 12.36 Vulval lichen planus: in this example of resolving disease, there are linear hyperpigmented lesions. By courtesy of the Institute of Dermatology, London, UK.

Fig. 12.37 Perineal lichen planus: typical papules with Wickham striae are present. By courtesy of the Institute of Dermatology, London, UK.

Fig. 12.38 Hypertrophic perianal lichen planus: chronic scratching has resulted in superimposed lichenification. By courtesy of the Institute of Dermatology, London, UK.

Fig. 12.39 Penile lichen planus: there is involvement of the shaft and glans. From Bunker C. Male Genital Skin Disease. Saunders Ltd./Elsevier 2004.

Fig. 12.40 Penile lichen planus: the proximal shaft shows post inflammatory hyperpigmentation. From Bunker C. Male Genital Skin Disease. Saunders Ltd./Elsevier 2004.

Fig. 12.41 Erosive lichen planus: bilateral erosions are present. By courtesy of the Institute of Dermatology, London, UK.
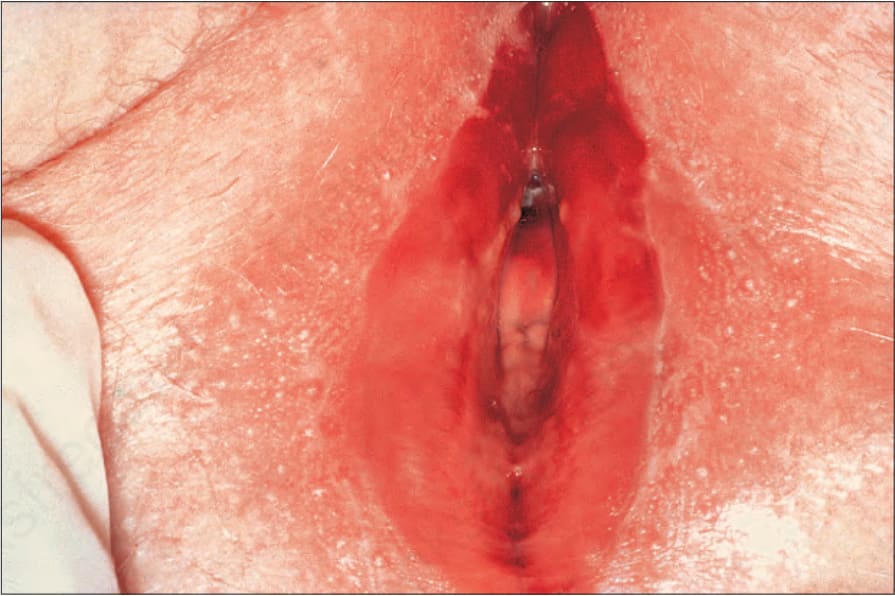
Fig. 12.42 Vulvovaginal-gingival syndrome: there is extensive vestibular erythema and erosion with a surrounding delicate white scale. By courtesy of the Institute of Dermatology, London, UK.
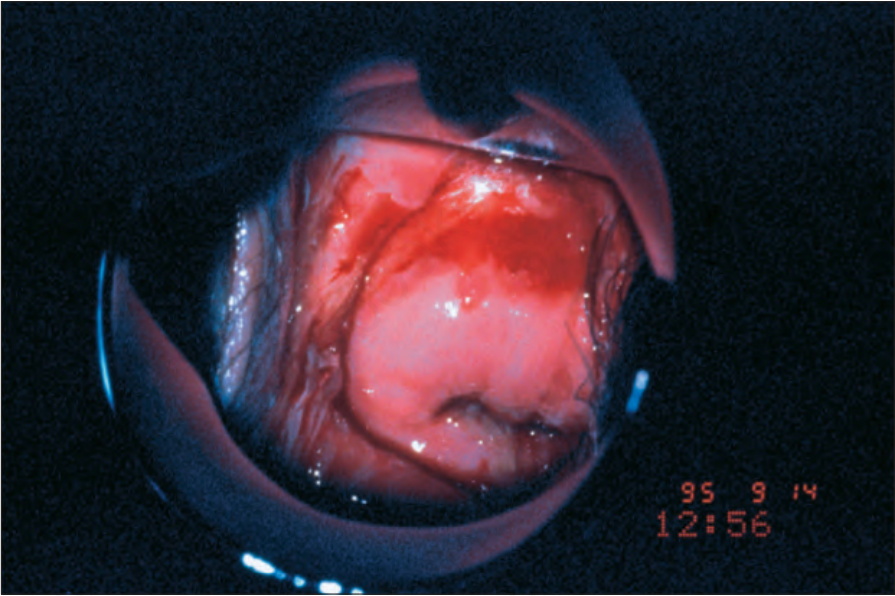
Fig. 12.43 Vulvovaginal-gingival syndrome: there is ulceration of the vagina and cervix. By courtesy of the Institute of Dermatology, London, UK.

Fig. 12.44 Vulvovaginal-gingival syndrome: note the intense erythema with erosion of the gum. By courtesy of the Institute of Dermatology, London, UK.

Fig. 12.45 Lichen planus: chronic penile lesion complicated by an ulcerated squamous cell carcinoma. By courtesy of the Institute of Dermatology, London, UK.
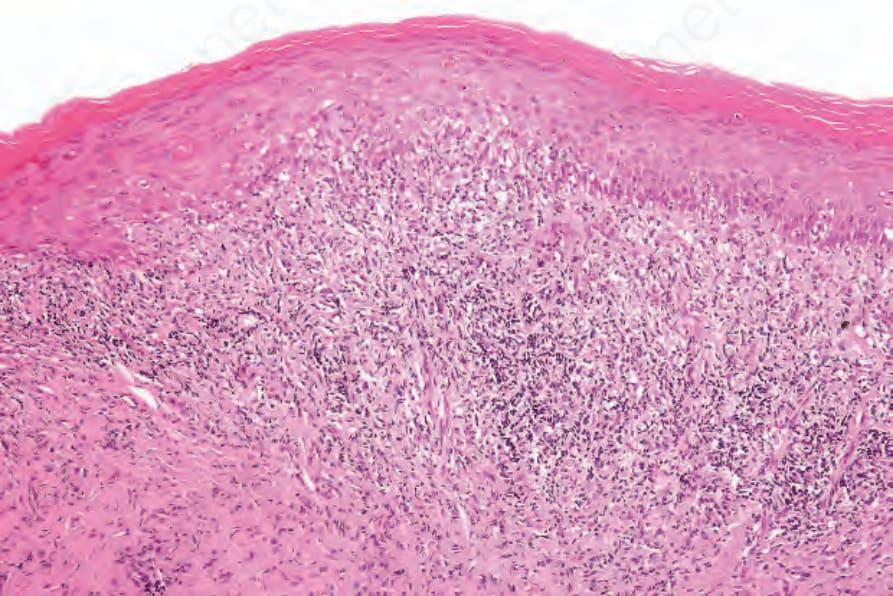
Fig. 12.46 Lichen planus: there is hyperkeratosis, acanthosis, and a bandlike inflammatory cell infiltrate.
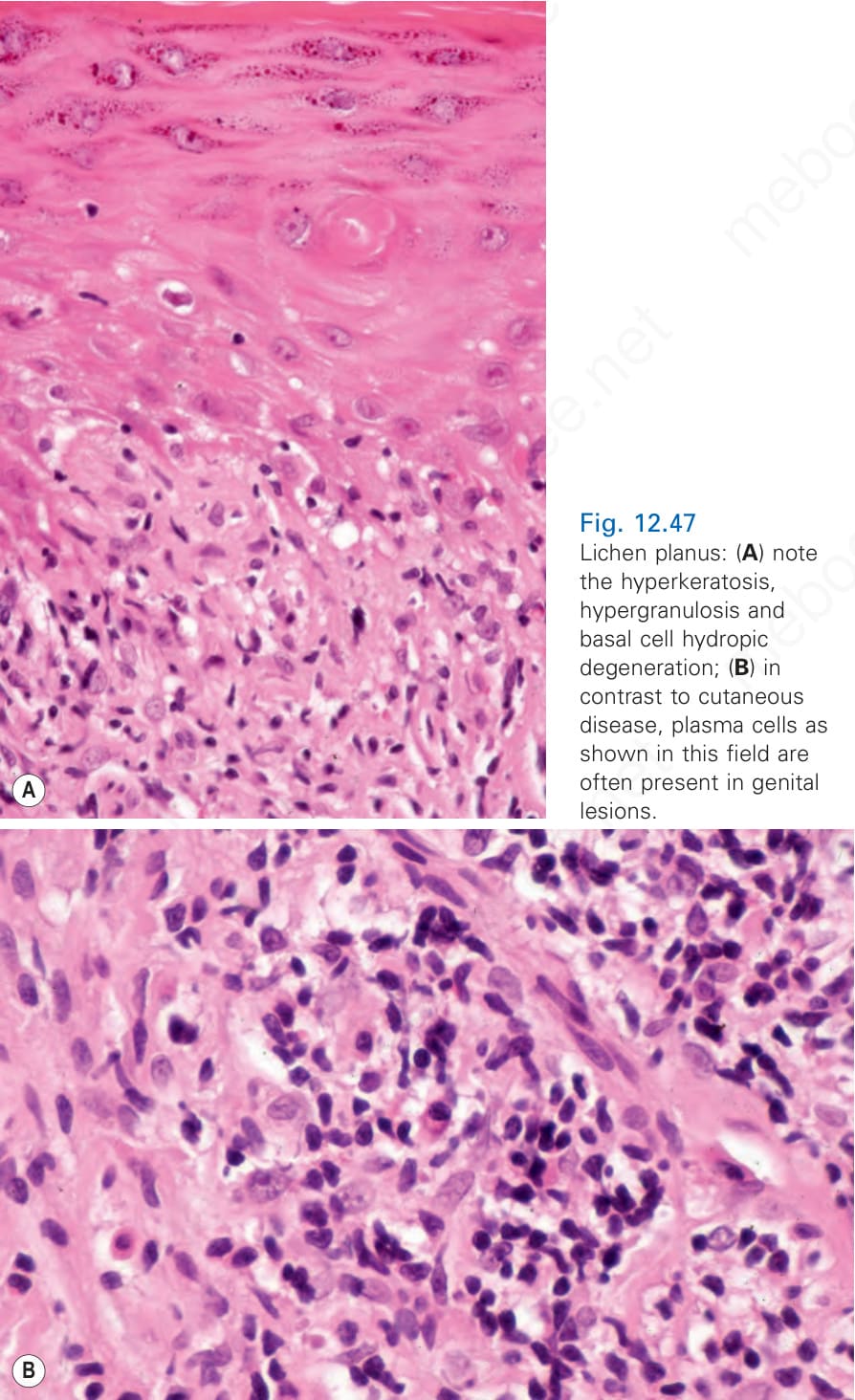
Fig. 12.47 Lichen planus: (A) note the hyperkeratosis, hypergranulosis and basal cell hydropic degeneration; (B) in contrast to cutaneous disease, plasma cells as shown in this field are often present in genital lesions.