Reactive arthritis
Reactive arthritis
Clinical features Reactive arthritis (previously known as Reiter syndrome) is part of the same continuum as psoriasis in genetically predisposed individuals.1 Reactive arthritis is defined by the triad of arthritis, urethritis, and conjunctivitis. It is precipitated by non-specific urethritis, bacillary or amebic dysentery, and associated with HIV infection and the immunogenotype human leukocyte antigen (HLA) B27.2–6 The classical triad may occur together or develop in sequence, and a range of other symptoms may also be present. It has a worldwide distribution. Reactive arthritis most commonly affects men 20–30 years of age; the male/female sex ratio is approximately 10 : 1.1 The syndrome is characterized by a relapsing course.4
The condition may follow an enteric or a urogenital infection.7,8 Shigella dysentery was the first associated enteric infection to be recognized and the causative organisms were either Shigella flexneri or Shigella dysenteriae.9
Stomatitis and nail dystrophy (indistinguishable from that of psoriasis) may be additional features.4 Weight loss is common.20 Aortic incompetence is an important late complication, and immunoglobulin A (IgA) nephropathy has been described in a number of patients.4,33
Reactive arthritis is rarely reported in females. Vulvitis has been described in a small number of case reports,34–38 and in one case cervical lesions, presenting as white papules, were seen.37 The vulval lesions are erythematous and may be ulcerative, eroded, or scaly, and often resemble mucocutaneous candidiasis.
Reactive arthritis may resolve spontaneously, but more often it is characterized by chronicity and recurrences.4 Rarely, it may prove fatal.4 Causes of death include aortic incompetence, atrioventricular block, terminal cachexia, systemic amyloidosis, and iatrogenic effects.39
481 Inflammatory dermatoses
482 Diseases of the anogenital skin
Patients present with systemic symptoms and variable skin lesions including folliculitis, vasculitis, acneiform eruptions, vesiculopustules, and erythema nodosum-like features.
Early joint lesions are characterized by a neutrophil polymorph inflammatory cell infiltrate with little, if any, synovial changes. Older lesions show features suggestive of rheumatoid arthritis, including lymphoid aggregates, a perivascular chronic inflammatory cell infiltrate, and synovial hyperplasia.30
Histologic features Essentially, just as the skin lesions of reactive arthritis have psoriasiform morphology (Fig. 12.31, they have the same histopathology and ultrastructure as pustular psoriasis.40
Differential diagnosis Periodic acid–Schiff (PAS) and/or silver stains should always be performed to exclude a fungal infection which can show similar histologic features.

Fig. 12.26 Reactive arthritis: there are bilateral keratotic papules and plaques affecting the soles of the feet. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.
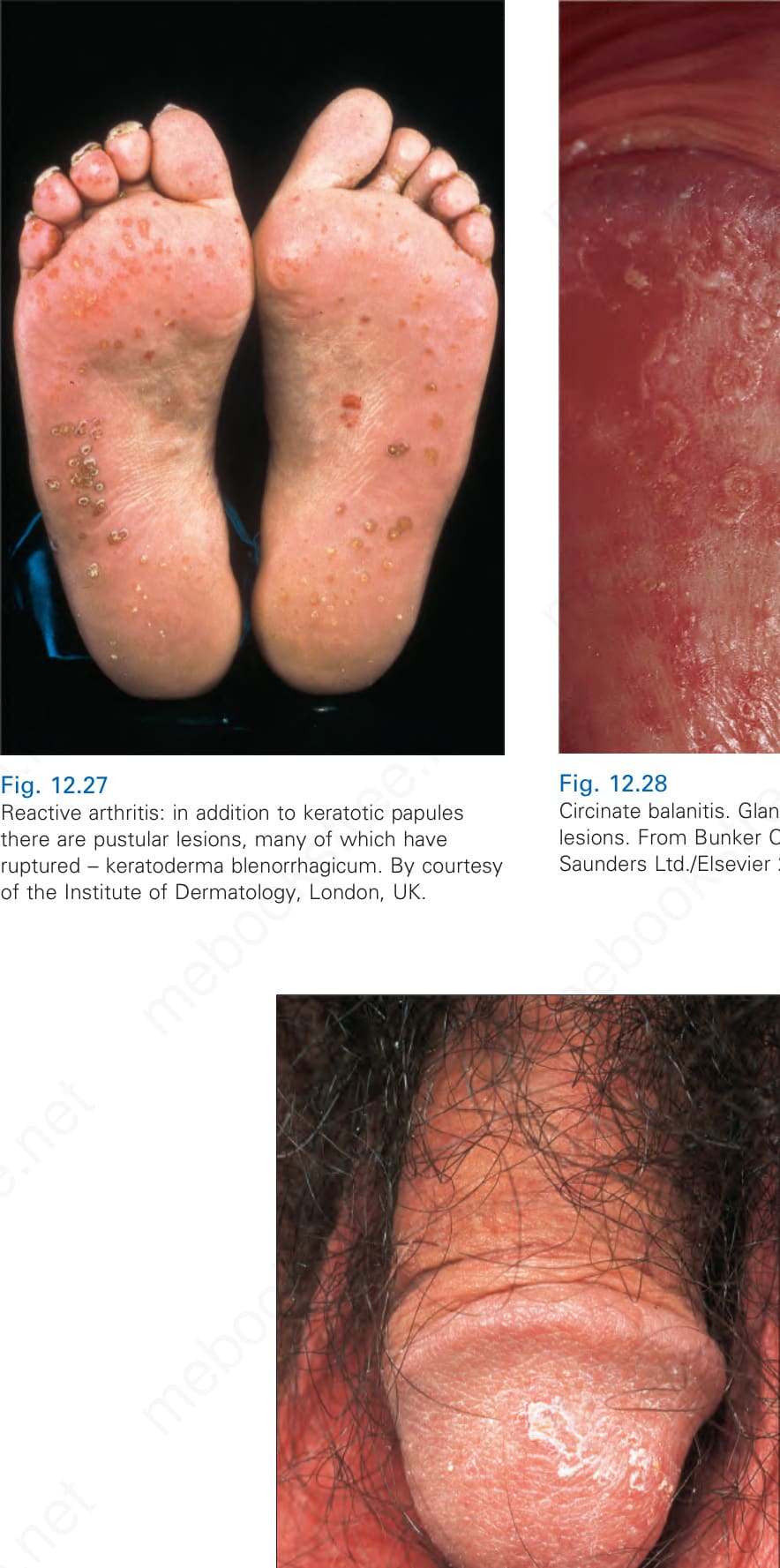
Fig. 12.27 Reactive arthritis: in addition to keratotic papules there are pustular lesions, many of which have ruptured – keratoderma blenorrhagicum. By courtesy of the Institute of Dermatology, London, UK.

Fig. 12.28 Circinate balanitis. Glans penis. Psoriasiform lesions. From Bunker C. Male Genital Skin Disease. Saunders Ltd./Elsevier 2004.

Fig. 12.29 Reactive arthritis: there are multiple erosions on the glans penis. By courtesy of the Institute of Dermatology, London, UK.

Fig. 12.30 Reactive arthritis: in this patient, there are scaly lesions on the glans penis. By courtesy of the Institute of Dermatology, London, UK.
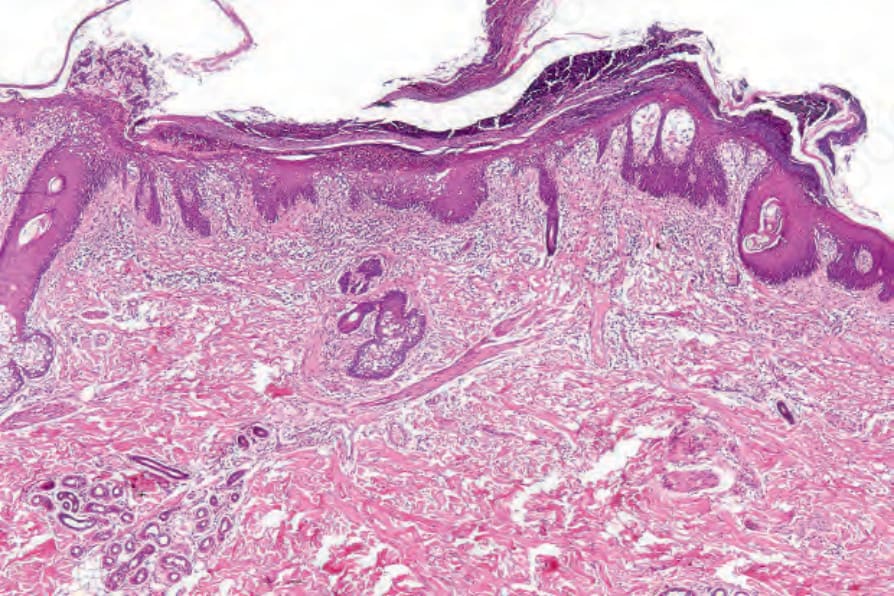
Fig. 12.31 Reactive arthritis: there is parakeratosis overlying a macropustule. The squamous epithelium shows psoriasiform hyperplasia. These features are indistinguishable from pustular psoriasis.
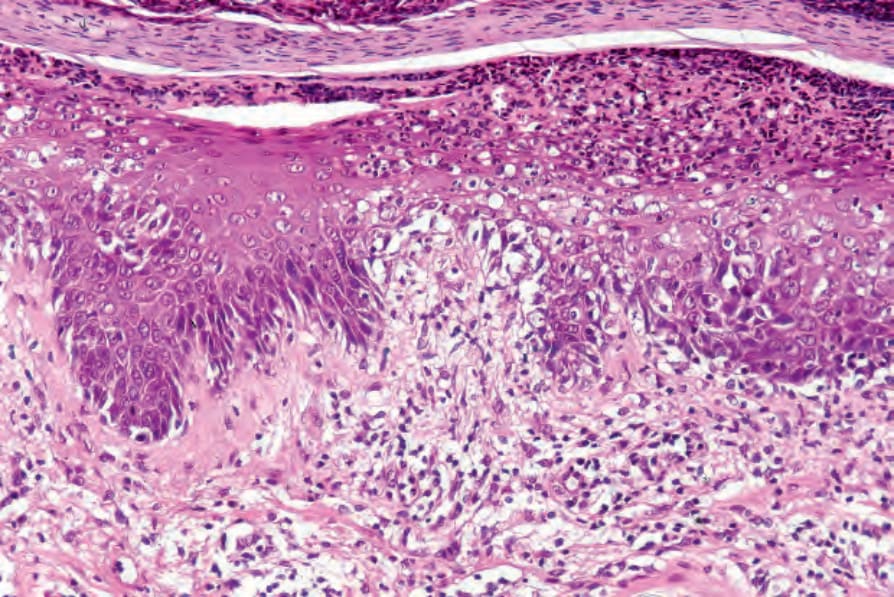
Fig. 12.32 Reactive arthritis: high-power view showing parakeratosis and a pustule.

Fig. 12.33 Lichen planus: perineal lesions showing conspicuous striae. By courtesy of the Institute of Dermatology, London, UK.