Calciphylaxis
Calciphylaxis
Clinical features Calciphylaxis was originally defined by an experimental model in rats, in which sensitization with parathormone or dihydrotachysterol followed by the injection of a challenging agent such as a metal salt resulted in localized
Calciphylaxis presents clinically as an often bilateral and symmetrical, pruritic, and frequently painful/tender eruption most often affecting the lower limbs (Fig. 10.65). Less often, lesions may affect the breasts, buttocks, abdomen, and penis.8–24 Calciphylaxis shows female predominance (about 2 : 1) and most commonly develops in the fifth decade of life.25 Lesions are often well-delineated, livedoid, violaceous plaques and nodules associated with ischemic necrosis of the underlying tissues, sometimes extending down to the fascia. Ulceration is typically present, and sometimes bullae are a feature. Gangrene and autoamputation may accompany acral involvement.6 Intestinal involvement with massive hemorrhage has exceptionally been documented.16
Calciphylaxis is associated with considerable morbidity and a high mortality of up to 60%.4,14,26 The majority of patients succumb to secondary infection. Calciphylaxis due to the end-stage kidney disease can exceptionally develop in children.27
371 Calciphylaxis
Pathogenesis and histologic features
The precise mechanism by which the subcutaneous vasculature undergoes calcification is uncertain but is probably multifactorial. In the majority of patients, however, sensitization occurs as a consequence of abnormal calcium/phosphorus metabolism in a setting of chronic renal failure and secondary or tertiary hyperparathyroidism. Frequently, the patients are undergoing dialysis. Less often, there is a background of primary hyperparathyroidism or hypervitaminosis D.4,12,14,17 Although in many patients calcium deposition occurs in association with an increased calcium-phosphorus product, in a significant proportion of patients calcium and phosphorus levels are normal.4 It has been suggested that in such patients the calcification develops as a direct response to excess parathormone or vitamin D. Challenging agents resulting in the vascular precipitation of calcium salts are unknown, but a number of substances (including albumin, corticosteroids, warfarin, and immunosuppressives) have been incriminated.12,28–30 Calciphylaxis has also been described in association with decreased functional protein C.13 Rarely, the condition has presented in a patient with no evidence of a renal disorder or increase in parathormone level.17 Diabetes, obesity, autoimmune diseases (rheumatoid arthritis, systemic lupus erythematosus, antiphospholipid syndrome), malignant tumors, giant cell arteritis, as well as alcoholic liver disease have been implicated in these patients.25,31–38
Histologically, the characteristic feature is calcification of the small- to medium-sized arteries and arterioles (Figs 10.66 and 10.67). Calcified debris may sometimes be present within the lumina, and occasionally the vessels are thrombosed (Fig. 10.68). Intimal fibroblastic proliferation with luminal narrowing has also been described (Fig. 10.69).9 Hemorrhage within the subcutaneous fat may be seen and fat necrosis accompanied by a lobular lymphohistiocytic infiltrate has been documented in a number of cases (Fig. 10.70). Interstitial calcification is only rarely a feature.9 Exceptionally, pseudoxanthoma elasticum-like changes have been documented.39 In a related phenomenon, epidermal and follicular calcification have been described in the absence of vascular lesions in a patient with toxic epidermal necrolysis in a background of hyperparathyroidism.40
Differential diagnosis Calcification involving small arteries and arterioles not accompanied by thrombosis has been described in patients with nephrogenic systemic fibrosis.41 Furthermore, incidental vascular calcifications can also be found in patients with peripheral vascular disease, renal insufficiency, and diabetes mellitus.42
372 Inflammatory diseases of the subcutaneous fat

Fig. 10.65 Calciphylaxis: ulcerated gangrenous lesion with surrounding erythema. By courtesy of A. Qureshi, MD, Department of Dermatology, Brigham and Women’s Hospital, Boston, USA. cutaneous extravascular lesions are predominantly seen in patients with secondary disease.21
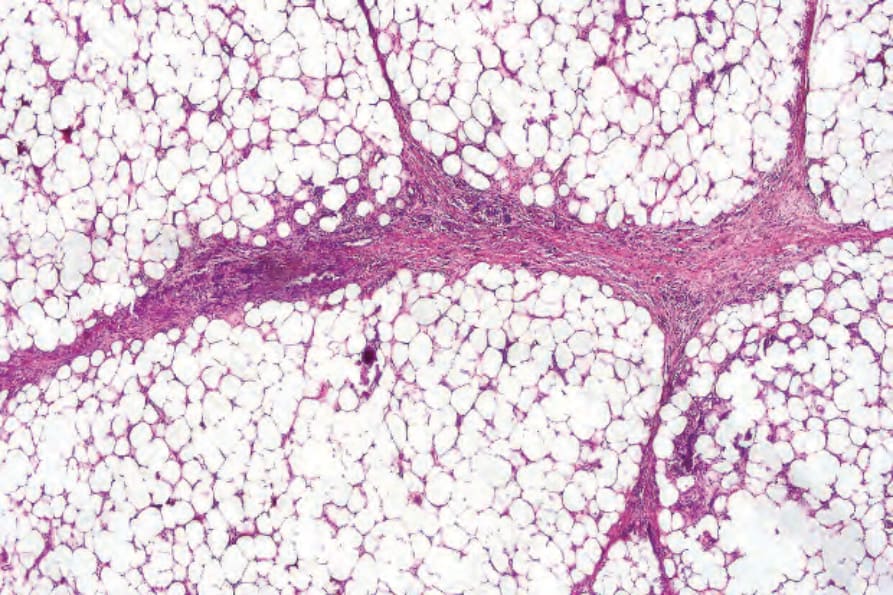
Fig. 10.66 Calciphylaxis: there is focal fat necrosis and widespread calcification affecting the small vessels. Note the thickened and fibrosed septa.
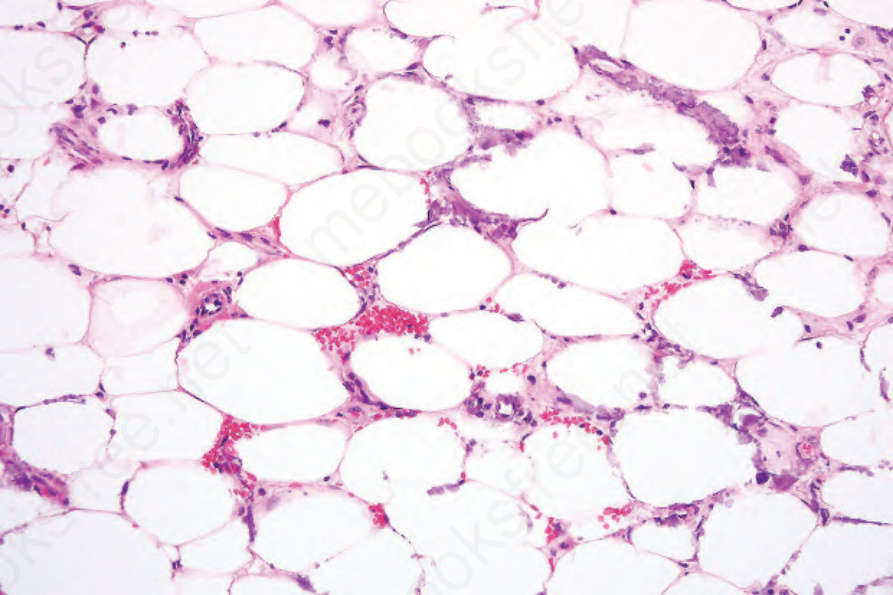
Fig. 10.67 Calciphylaxis: calcification of the small vessels and capillaries within the subcutaneous fat is evident.
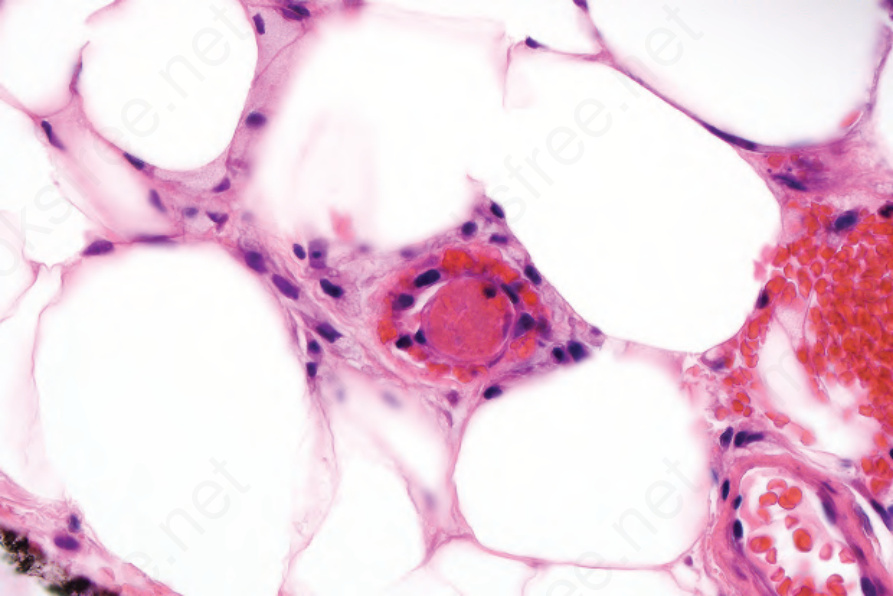
Fig. 10.68 Calciphylaxis: note the thrombosed vessel in the center of the field.
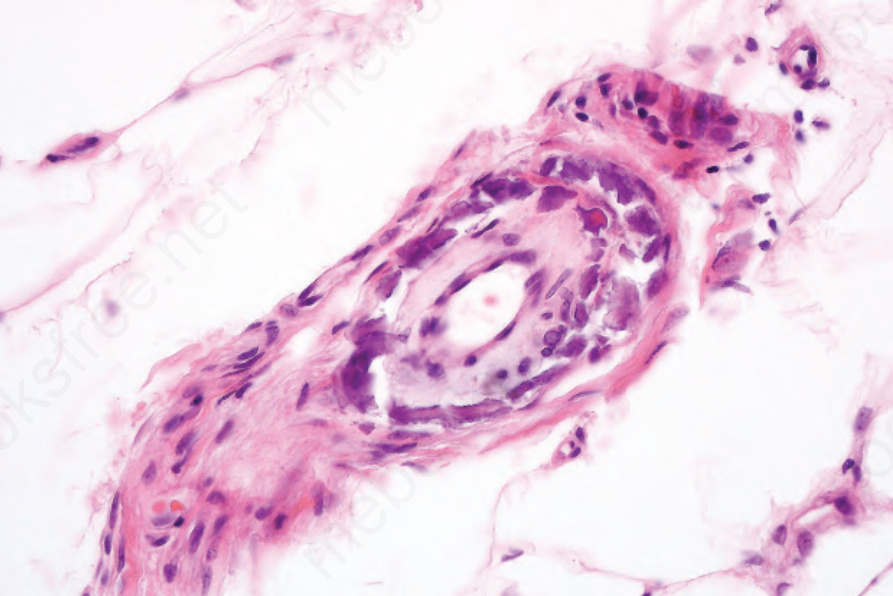
Fig. 10.69 Calciphylaxis: in addition to mural calcification, there is marked intimal fibroblastic proliferation.
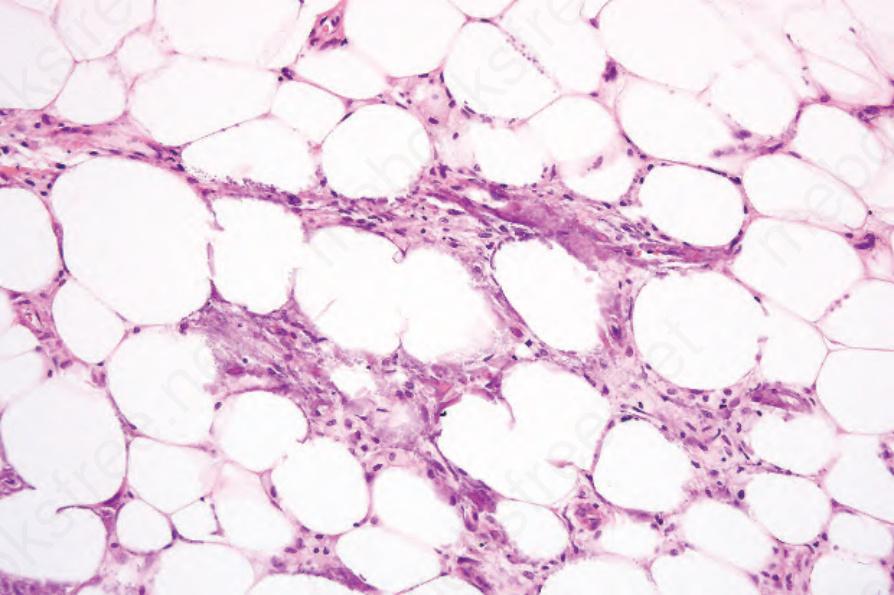
Fig. 10.70 Calciphylaxis: fat necrosis with conspicuous lipophages. In addition, there is widespread calcification.