Acne agminata
Acne agminata
of lesions is due to an unusual granulomatous reaction to ruptured hair follicles.15
The histologic features vary with the stage of evolution and may be entirely non-specific.16 A biopsy from a well-established lesion shows a central area of well-defined caseous necrosis surrounded by multinucleate giant cells and epithelioid cells (sometimes indistinguishable from tuberculous infection) (Figs 9.98 and 9.99). Serial sections often reveal a relationship of the necrosis to a destroyed hair follicle. Sarcoidal granulomas may be a feature. Special stains may demonstrate a ring of elastic fibers in the center of the necrotic focus, possibly representing the isthmus of the hair follicle. The granulomata are not usually related to Demodex folliculorum as is often the case in granulomatous rosacea. Lymphagiectasia is often a feature.7 Focal vasculitis is only exceptionally seen.
Clinical features Acne agminata (lupus miliaris disseminatus faciei, acnitis, papular tuberculid) is a rare condition originally thought to be a form of tuberculid, but an association with tuberculosis has since been excluded.1–4 Some authors consider this disease to be synonymous with granulomatous rosacea. However, the distinctive clinical presentation, and the absence of typical rosacea in patients affected by the disease, argue against this. Recently, a new name has been suggested for the disease: facial idiopathic granulomata with regressive evolution (FIGURE).5
Clinical presentation is characterized by fairly monomorphous yellowish-brown papules typically involving the central face with predilection for periocular areas (Fig. 9.97). The disease is limited to the eyelids and canthus in rare cases.6,7 Involvement of axillae or upper limbs is an exceptional finding.8–11 There is no sex predilection, and the age range is wide although most cases occur in young to middle-aged adults.12 An exceptional case during pregnancy has been documented.13 Response to conventional treatment for rosacea is often ineffective, but lesions tend to regress spontaneously over a period of months or even years, leaving mild scarring.14
Differential diagnosis The diagnosis is fairly easy in the presence of granulomata surrounding an area of caseation necrosis since the latter is not usually a feature of either granulomatous rosacea or perioral dermatitis. In biopsies showing only focal granulomatous inflammation, establishing the diagnosis may require very careful clinicopathological correlation. In idiopathic facial aseptic granuloma which is a self-limited condition that may related to granulomatous rosacea and presents in children as one or several facial papules/nodules, the granulomas are of the foreign body type and necrosis is not seen.17,18
Pathogenesis and histologic features As suggested by some synonyms, infection by mycobacteria has been favored by certain authors as a potential etiological factor. This theory is no longer tenable due to the absence of past or present systemic tuberculosis and the constant failure of isolation of bacilli. In a study from Israel, mycobacterial DNA was not detected by PCR.1 It has been suggested that the development

Fig. 9.97 Acne agminata: note the characteristic distribution of papules on the cheek and around the eyes. From the collection of the late N.P. Smith, MD, the Institute of Dermatology, London, UK.
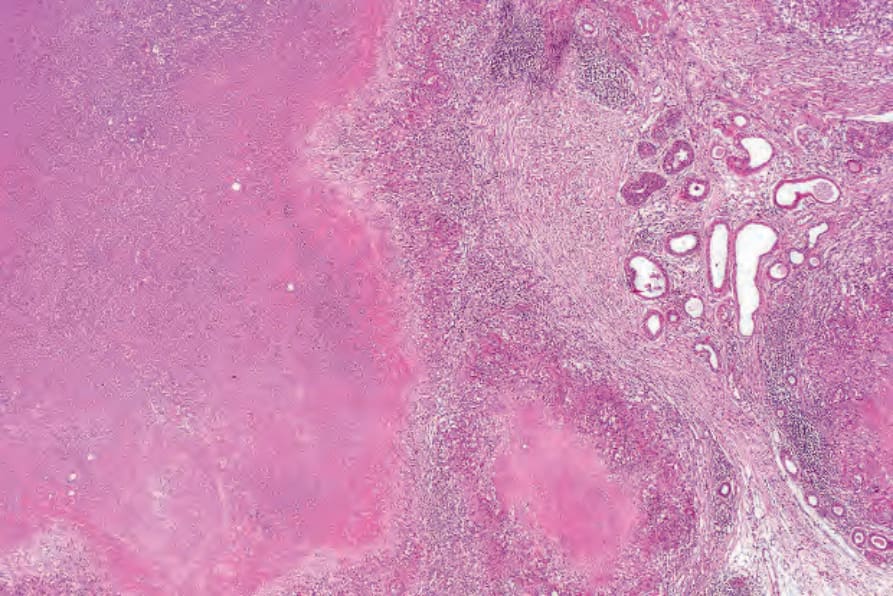
Fig. 9.98 Acne agminata: there are multiple caseating granulomata.
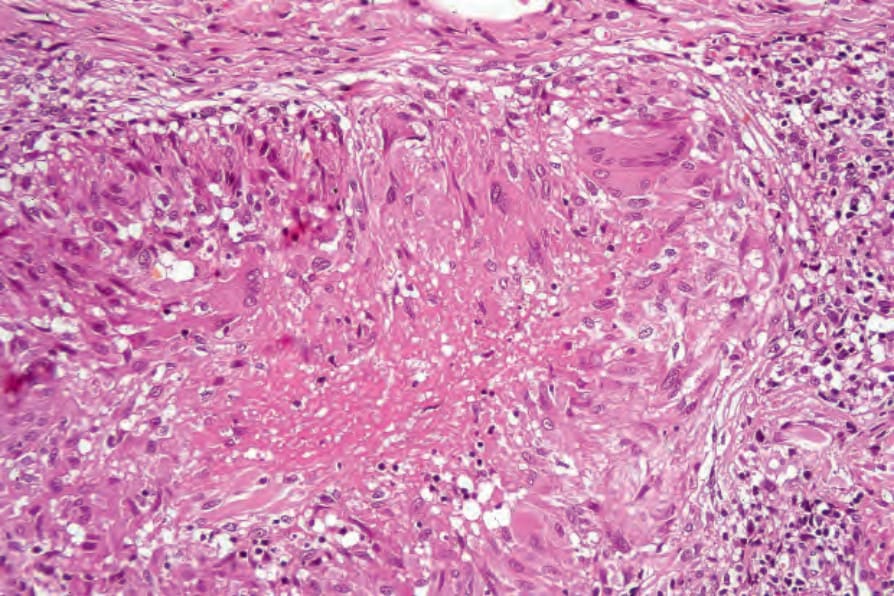
Fig. 9.99 Acne agminata: close-up view. The condition is not a tuberculid. Special stains and culture for tubercle bacilli are invariably negative.