Necrobiotic xanthogranuloma
Necrobiotic xanthogranuloma
Clinical features Necrobiotic xanthogranuloma (necrobiotic xanthogranuloma with paraproteinemia) is an extremely rare condition of unknown etiology.1–3 It occurs equally in men and in women, in the late middle aged and elderly (average age at presentation is 56 years). The disease is characterized by the development of nodules and plaques, which show a predilection for the face, neck, trunk, and, less commonly, proximal limbs. Lesions limited to single body site are rarely seen. The facial lesions are characteristically periorbital (most
The lesions on the trunk and limbs are irregular, well-demarcated, bright yellow, dermal and subcutaneous plaques measuring up to 25 cm across (Fig. 9.88). They may be complicated by ulceration, hemorrhage, scarring, central atrophy, and telangiectases, and typically have a peripheral inflammatory border. Violaceous and flesh-colored nodules are sometimes present, particularly over the trunk. Unusual presentations include a solitary nodular lesion mimicking a tumor and, exceptionally, the absence of skin involvement.8,9 A lesion presenting at the site of a blepharoplasty scar and a further lesion presenting in the scar of a burn have been reported.10,11
Involvement of myocardium, lung, larynx, kidneys, salivary gland, skeletal muscle, oral mucosa, and vulva has been documented.12–19 Patients may have arthritis, chronic obstructive pulmonary disease, neuropathy, or
hypertension.2 Other reported cases include one associated with Graves disease, another with linear morphea, one with scleroderma, and one with lichen sclerosus.2,20–22 In rare patients, there was an association with syncitial giant cell hepatitis and with autoimmune immunoglobulin G4-related pancreatitis.23–25 Nodular transformation of the liver is a feature noted in rare patients.15,26 A single patient also had associated normolipemic xanthomatosis.18
Laboratory investigations reveal anemia, leukopenia, and a raised ESR. Most patients with necrobiotic xanthogranuloma have an associated monoclonal paraproteinemia of uncertain significance (MGUS), usually IgG kappa type (60% of cases). Few present with a lambda paraprotein and an exceptional case has been documented with two monoclonal paraproteins. An association with Waldenström macroglobulinemia is exceptional.27 There is an important association with multiple myeloma, and the latter can develop many years after the diagnosis of the disease.28 Other associations include B-cell lymphoma and chronic lymphocytic leukemia.29–34 A case with associated Hodgkin lymphoma has also been reported.35 Diabetes mellitus is sometimes present and occasionally, hyperlipidemia. Other associations that may be encountered include low serum complement levels and cryoglobulinemia.
333 Necrobiotic xanthogranuloma
Pathogenesis and histologic features The pathogenesis of necrobiotic xanthogranuloma is unknown. The plasma cells in the infiltrate are consistently polyclonal, supporting a reactive process.3 Direct immunofluorescence has shown IgM, C3, and fibrinogen deposition in blood vessel walls.6 It has more recently been suggested that activation of monocytes is responsible for the intracellular accumulation of lipoprotein-derived lipids and the hypocholesterolemia.36 Focus-floating microscopy of six cases demonstrated the presence of Borrelia.37 The significance of this finding is unclear, but it is unlikely that the bacteria plays a pathogenetic role in the disease.
Necrobiotic xanthogranuloma has a very distinctive histologic appearance.8,33 Large areas of marked necrobiosis alternate with foci of xanthogranulomatous infiltration throughout the reticular dermis with extension into the subcutaneous fat (Fig. 9.89).4 Exceptionally, necrobiosis is absent.38 Involvement of the subcutaneous fat is predominantly in a septal distribution and can mimic panniculitis.39 The necrobiotic collagen appears as amorphous eosinophilic debris (Fig. 9.90). The granulomatous infiltrate is composed of epithelioid and foamy histiocytes in addition to conspicuous giant cells, many of which are of the Touton type (Figs 9.91 and 9.92). Foreign body giant cells are also present. Lymphocytes and plasma cells are often prominent and formation of germinal centers is sometimes seen. A characteristic feature is the presence of large and bizarre angulated giant cells with considerable numbers of nuclei irregularly grouped together
334 Granulomatous, necrobiotic and perforating dermatoses
multinucleated giant cells, and Touton-type giant cells distinguishes necrobiotic xanthogranuloma from necrobiosis lipoidica and other necrobiotic dermatoses. It should, however, be noted that prominent cholesterol cleft formation may rarely be seen in necrobiosis lipoidica.46 Adipophilin staining has been reported as being of use in the differential diagnosis between both conditions. In necrobiotic xanthogranuloma, the staining pattern is diffuse, highlighting the necrobiotic and cellular areas. In necrobiosis lipoidica, however, the staining is restricted to necrobiotic areas.47,48 Small punch biopsies may not be adequate for definitive evaluation and sampling bias may be misleading. Clinical correlation should be taken into consideration before making a definitive diagnosis.

Fig. 9.88 Necrobiotic xanthogranuloma: there are multiple yellow plaques around the shoulders and overlying the clavicles. By courtesy of the Institute of Dermatology, London, UK.
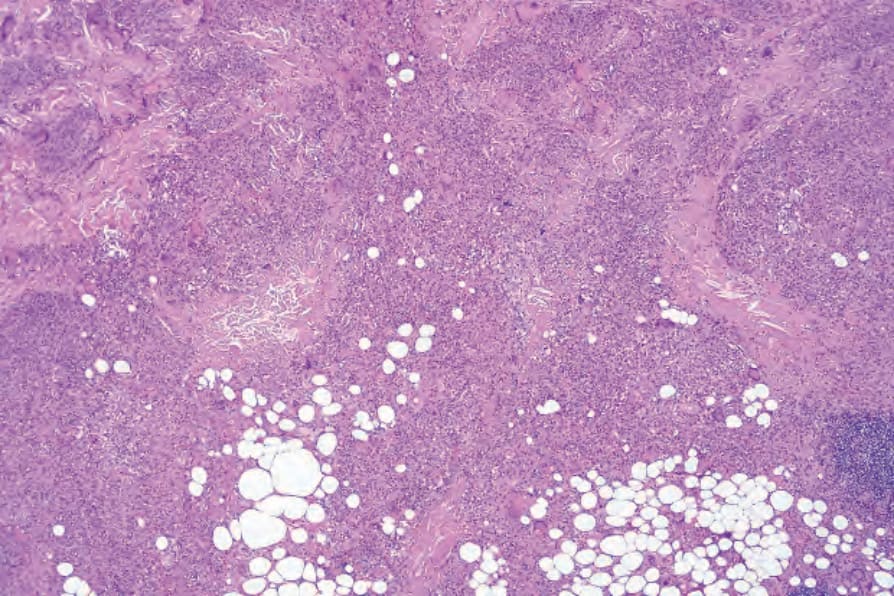
Fig. 9.89 Necrobiotic xanthogranuloma: there is a dense infiltrate extending throughout the dermis into the subcutaneous fat.
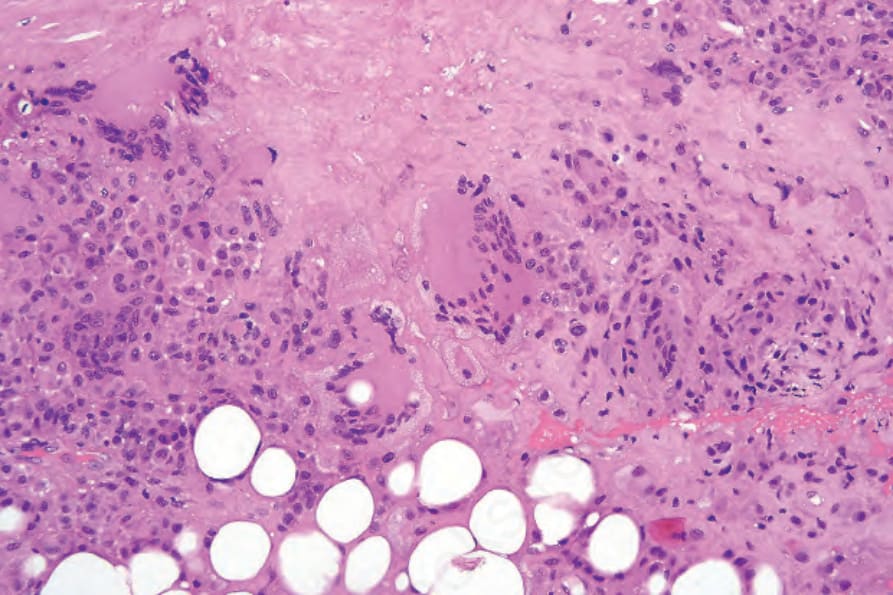
Fig. 9.90 Necrobiotic xanthogranuloma: there is extensive necrobiosis and a dense histiocytic infiltrate with conspicuous giant cells.
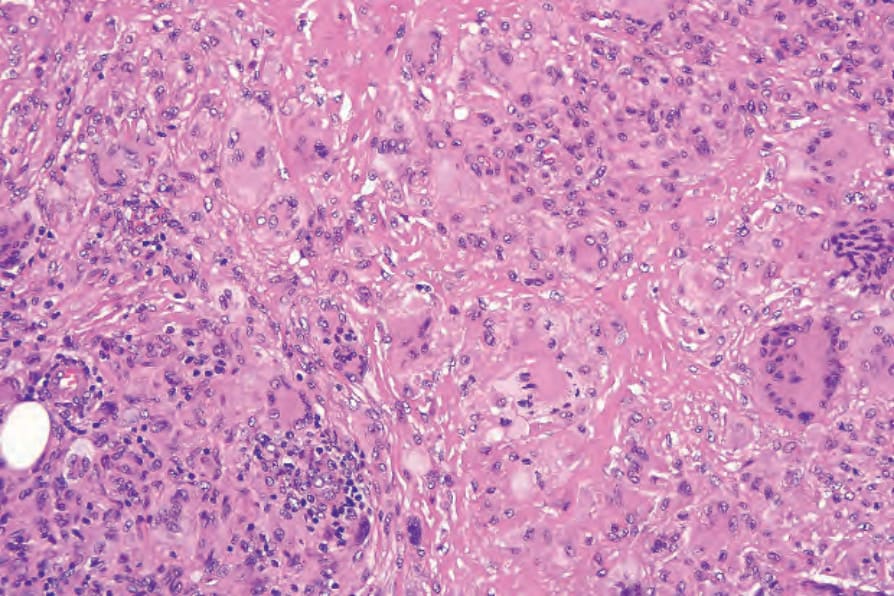
Fig. 9.91 Necrobiotic xanthogranuloma: in this field, there are conspicuous xanthomatized histiocytes.
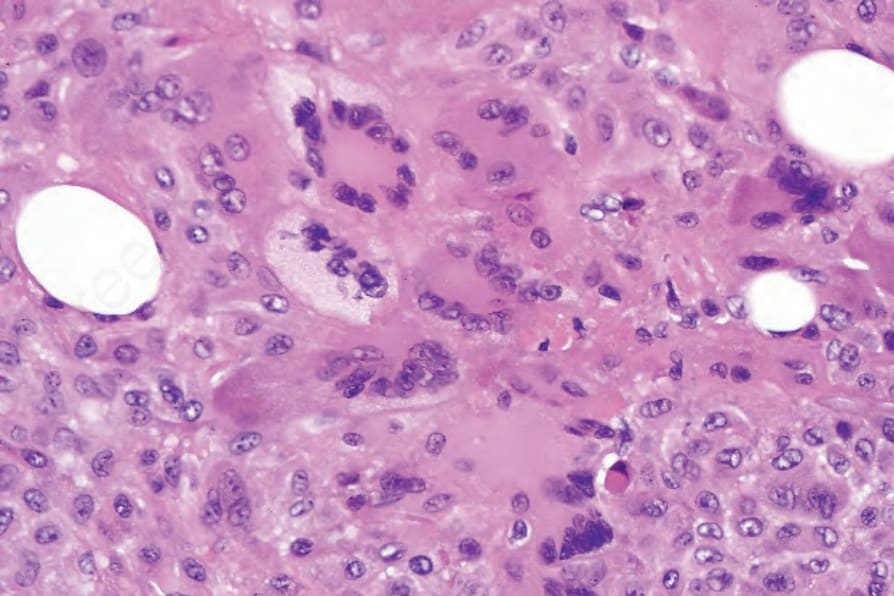
Fig. 9.92 Necrobiotic xanthogranuloma: Touton giant cells are sometimes prominent.
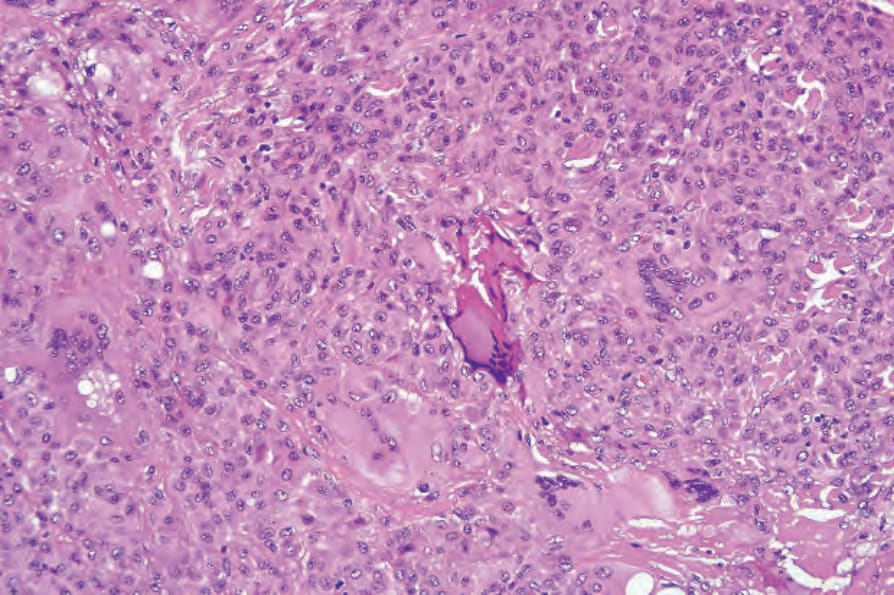
Fig. 9.93 Necrobiotic xanthogranuloma: angulated giant cells with darkly staining nuclei are commonly present.