Actinic granuloma (O’Brien)
Actinic granuloma (O’Brien)
Clinical features Actinic granuloma develops on the sun-damaged skin of the neck, face, upper chest, or arms of middle-aged patients.1–5 It may also affect the conjunctiva, and a single case affecting the upper lip has been reported.6–9 Lesions restricted to the conjunctiva of young women are exceptional.10 A further case presented as alopecia.11 The incidence is equal in men and women, and individuals with blond hair and freckled skin are predisposed, particularly those living in sunny climates. An association with the long- standing use of sunbeds and with doxycycline phototoxicity has also been described.12,13
Annular elastolytic giant cell granuloma (annular elastolytic granuloma)
Clinical features The term ‘annular elastolytic giant cell granuloma’ has been used to describe not only cases of actinic granuloma but also lesions in which destruction of elastic fibers occurs in the absence of solar elastosis.6 In fact, some cases present at sites with little sun exposure and the disease may also occur in children.7 Thus, although the terms actinic granuloma, elastolytic giant cell granuloma, and even elastolytic actinic giant cell granuloma have been used interchangeably in the literature, the latter term should be reserved for elastolytic granulomata occurring in skin without solar elastosis but not restricted to covered skin.8,9
Lesions present as one or more skin-colored or pink papules, which enlarge to form annular or arcuate plaques up to 1 cm in diameter. The edge of the lesion is somewhat raised, forming a border 0.2–0.5 cm in width. These annular plaques enlarge slowly, and the center may gradually clear to appear relatively normal or slightly atrophic with variable depigmentation. Lesions are asymptomatic and there is no evidence of anesthesia. However, there is usually clinical exacerbation associated with sun exposure.14 They do not develop on non-sun-damaged skin. Spontaneous resolution may take place after months or years.
Lesions usually present on the trunk and neck and rarely on proximal limbs. They vary in size but tend to be large. Despite the name annular, some cases present with papules or reticular erythema.10 In those that are annular, there is an advancing raised border which may be papular. Rarely, lesions are generalized and in one of such cases, the lesions spared the striae distensae.11,12 Spontaneous resolution is rare.10 A reported case describes a lesion that developed at the site of an old burn scar and spread after trauma.13 In a single report, repigmentation of the gray hairs within the affected area of the scalp has been described, and in a further case the granulomas developed on lesions of vitiligo.14,15
Elastolytic granulomata have rarely been described in association with adult T-cell leukemia lymphoma, primary cutaneous CD4-positive small/ medium-sized pleomorphic T-cell lymphoma, acute myelogenous leukemia, monoclonal gammopathy, Hashimoto thyroiditis, temporal arteritis in one case following herpes zoster infection, squamous cell carcinoma of the tonsil, late-onset X-linked dominant protoporphyria, diabetes mellitus, and prostatic cancer.16–24 A unilateral lesion developing in a hemiplegic stroke patient has been reported, and in a further patient the lesion developed after the implantation of a pacemaker.25,26 Elastolytic granulomata have also been documented in internal organs.27 The latter, however, probably represents sarcoidosis with prominent elastolysis.
Bilateral periocular actinic granulomata have been documented in a patient with renal failure.15 Other rare associations likely to be coincidental include relapsing polychondritis, cutaneous amyloidosis, giant molluscum contagiosum, chronic lymphocytic leukemia, and erythema nodosum.16–20
Pathogenesis and histologic features The pathogenesis of actinic granuloma is poorly understood. It has been suggested that the antigenic stimulus for the formation of granulomata in both actinic granuloma and temporal arteritis is actinically degenerated elastic tissue.21,22 Interestingly, phototesting in a single case failed to reproduce the lesions of actinic granuloma.23
Pathogenesis and histologic features Elastic fibers become altered through an unknown mechanism and appear to induce factor XIIIa-positive cells and CD68-positive macrophages to form granulomata.28
Histologic features may be identical to those of actinic granuloma (see below) except for the absence of solar elastosis. Ideally, in annular lesions the biopsy should be a wedge including the center, the advancing edge, and normal skin for comparison purposes. This is not always possible,
The features are best appreciated by examination of a radial biopsy through the edge of a lesion and including uninvolved skin.24,25 The epidermis may be normal or atrophic. The peripheral unaffected skin shows gross solar (actinic) elastosis (Figs 9.73–9.75). Within the rim of the lesion there is a foreign body giant cell reaction in association with, and engulfing, fragmented elastotic material (elastoclasis) (Figs 9.76 and 9.77).24,25 The granulomatous reaction is centered in the zone of solar elastosis and, accordingly, tends to be confined to the superficial dermis.26 The giant cells may contain asteroid bodies. There is an accompanying chronic inflammatory cell infiltrate composed of histiocytes, lymphocytes, and plasma cells. Necrobiosis is not a feature of this condition. Palisading of histiocytes is either absent or minimal and, if present, is related to the elastotic debris. Dermal mucin does not appear to be increased.24 Fibroblasts are scant and fibrosis is minimal. In the actinic granuloma, blood vessels appear normal. Within the central zone the collagen appears relatively normal, although it is more obviously
329 Elastolytic granulomata
horizontally aligned and may appear more closely packed than normal. Slight scarring is present in the central area where elastic tissue is absent.26
Differential diagnosis The facial location, presence of elastophagocytosis, and absence of necrobiosis aid in distinguishing actinic granuloma from other granulomatous lesions. The absence of dermal mucin, necrobiosis, and palisading granuloma and the presence of marked elastoclasis and mild scarring help to distinguish actinic granuloma from granuloma annulare, the disorder that it most resembles.16,27
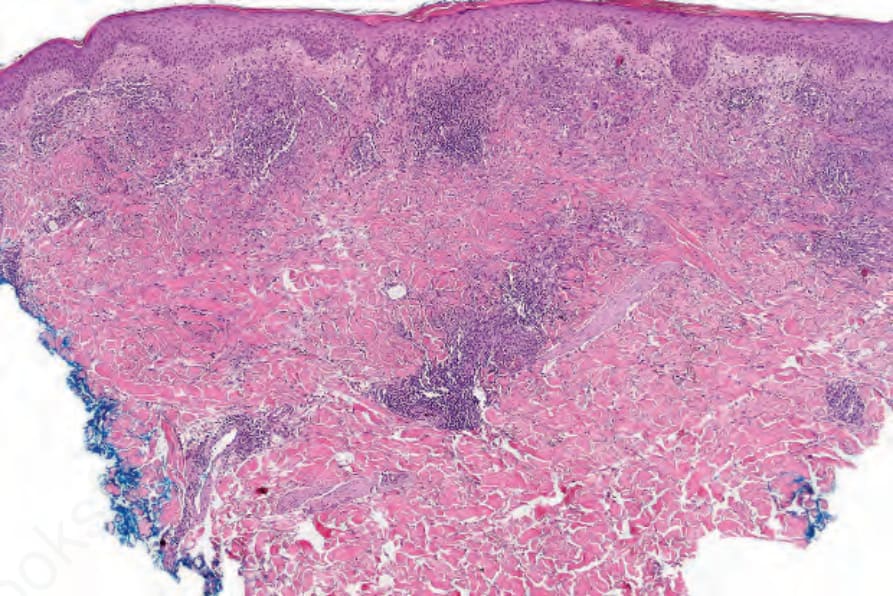
Fig. 9.73 Actinic granuloma: a granulomatous reaction is present the superficial dermis surrounding an ill-defined necrobiotic process. Solar elastosis is evident.
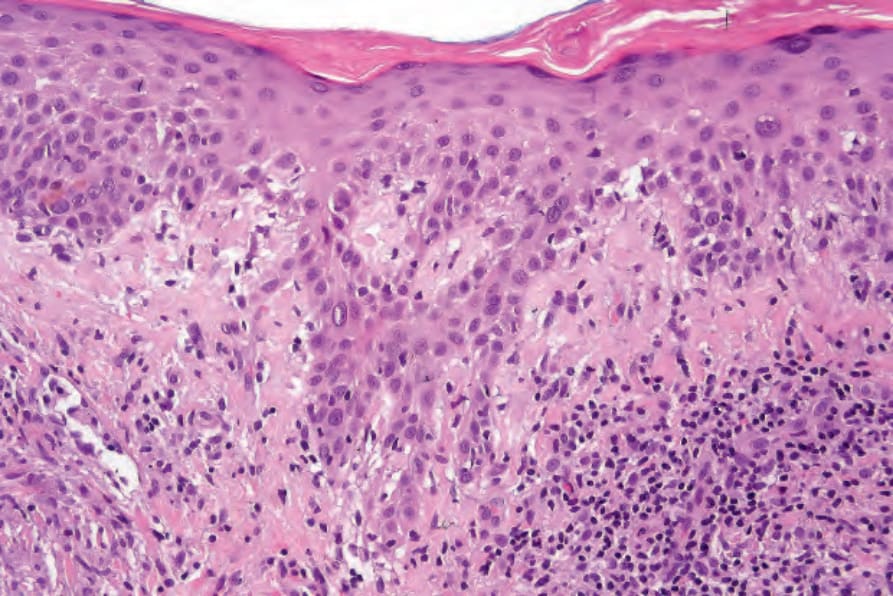
Fig. 9.74 Actinic granuloma: in addition to solar elastosis, this example also shows interface change with conspicuous cytoid bodies.
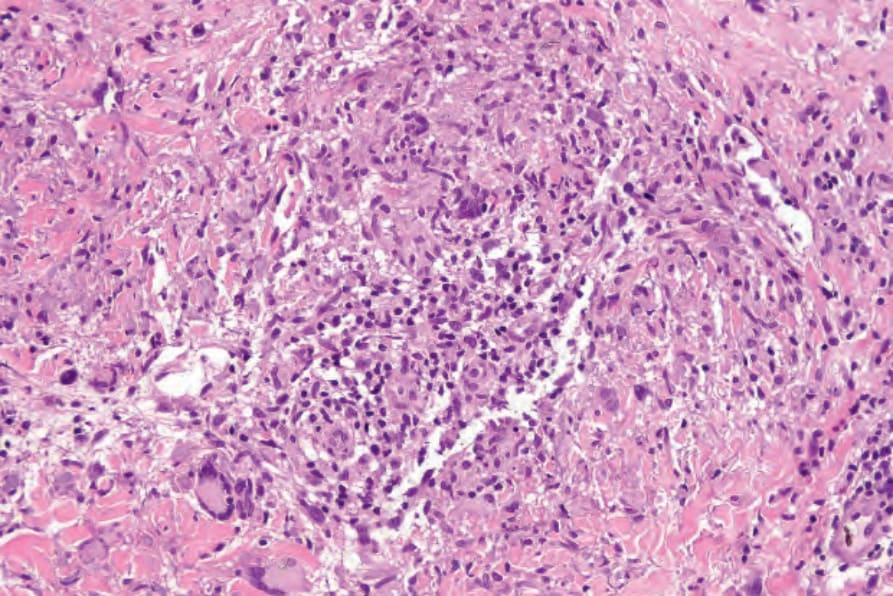
Fig. 9.75 Actinic granuloma: the granulomatous infiltrate is associated with degenerate elastic fibers.
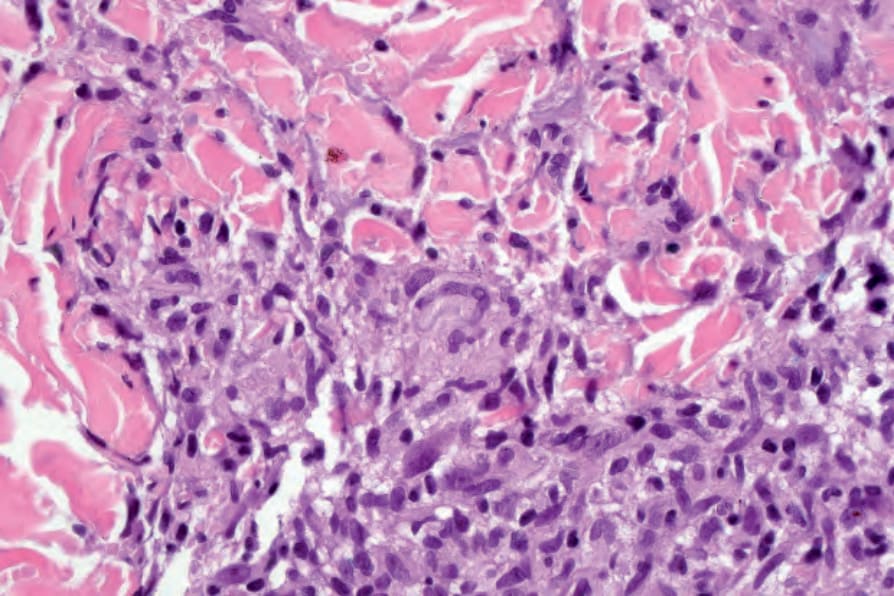
Fig. 9.76 Actinic granuloma: elastotic material is seen in the cytoplasm of the giant cell in the centre of the field.
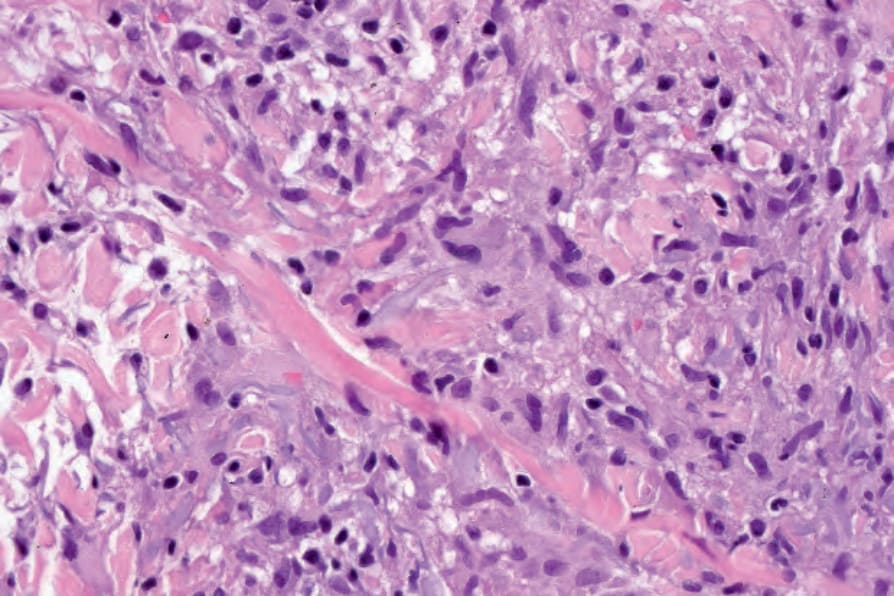
Fig. 9.77 Actinic granuloma: high-power view of basophilic degenerate elastic fibers.