Necrobiosis lipoidica
Necrobiosis lipoidica
Clinical features Necrobiosis lipoidica is a disease of unknown etiology which shows a strong association with diabetes mellitus.1–6 Although the affiliation is likely to have pathogenic implications, the precise mechanism by which the lesions of necrobiosis lipoidica develop is, nevertheless, unknown, and the nature of the relationship between the two diseases is unclear. Therefore, although the diagnosis of diabetes is most often established before the onset of the skin lesions (in up to 62% of cases), in a number of cases, typical plaques present simultaneously (in up to 24% of cases) or may precede (in up to 14% of cases) the apparent onset of diabetes mellitus by several years.2,7,8 The course of the cutaneous disease does not appear to be related to the hyperglycemia, and treatment of diabetes does not affect the outcome of the cutaneous lesions. In one study, proteinuria, retinopathy, and smoking were more common in patients with necrobiosis lipoidica compared with patients with diabetes but no skin disease.9 In another study, patients with diabetes type I and necrobiosis lipoidica tended to have higher levels of glycemia, and the duration of the diabetes was longer compared to patients without necrobiosis lipoidica.10 Interestingly, however, only a minority of patients with necrobiosis lipoidica has diabetes mellitus. It has been shown that 11% of patients with necrobiosis lipoidica have diabetes mellitus and a further 11% develop the disease or altered glucose tolerance on follow-up.11
reported in up to 13% of patients.30–32 It is more common in males and in those with diabetes mellitus.33 Perforating necrobiosis lipoidica is very rare and may be seen very exceptionally in children.34,35 In perforating cases, the clinical appearance may consist of a focal scaly depression or comedone-like lesions. Atypical forms may also be found: patients sometimes manifest papules and nodular lesions, and occasionally plaques resembling granuloma annulare are seen. (It should be noted, however, that rarely these two conditions appear to coexist.)16,36 Clinical presentations with papulonecrotic and noduloulcerative lesions mimicking gummata or erythema induratum have been documented, albeit exceptionally.30 The lesions may be solitary or multiple, often symmetrical, and show a predilection for the lower extremities, in particular, the pretibial area (Figs 9.50–9.53). They can also occur on the arms, hands, fingers, abdomen, nipples, and back; rarely, the face or scalp is affected, in which case diabetes is seldom present.37 Generalized lesions may exceptionally occur.38
Necrobiosis lipoidica may develop in both juvenile (type I) and maturity-onset (type II) diabetes. Interestingly, the condition improves or even resolves in diabetic patients after pancreatic transplant.12,13 Necrobiosis lipoidica has been documented in patients with endocrine disorders other than diabetes such as hypo- and hyperthyroidism, and also in association with inflammatory bowel disease and vasculitis.14 One nondiabetic patient with necrobiosis lipoidica and ataxia telangiectasia has been reported.15 Exceptionally, necrobiosis lipoidica and granuloma annulare have presented simultaneously.16,17 The disease has also been documented in association with sarcoidosis.18,19
Necrobiosis lipoidica shows a marked female preponderance (3.3 : 1), and although a wide age range may be affected, patients present most often in the fourth decade (those associated with diabetes mellitus) or fifth decade (those not associated with diabetes mellitus). The condition is rare in childhood and is often associated with diabetes mellitus. It also appears to be related to underlying renal and retinal disease.20–24 Familial cases may also occur, with or without diabetes.25–27 A case of monozygotic twins with diabetes mellitus type II and necrobiosis lipoidica has been reported.28
The so-called atypical necrobiosis lipoidica of the face and scalp does not represent a variant of necrobiosis lipoidica, and it is more likely to represent a variant of elastolytic granuloma (see page 329). The name was chosen because of the coexistence of typical lesions of necrobiosis lipoidica on the shins of one of the patients in the original series. However, most patients do not present with classic lesions of necrobiosis lipoidica elsewhere and the microscopic findings do not resemble the latter entity.39
The characteristic lesion, sometimes referred to as a sclerodermatous plaque, is round or oval, circumscribed, and often has a slightly elevated rim. It is typically a few millimeters to several centimeters in diameter. Newly acquired lesions are often red-brown in color, but with progression the center of the lesion becomes yellowish and the peripheral border may acquire a violaceous hue. Larger plaques are usually irregular and more variably shaped. Scaling and telangiectasia may become evident. Dermoscopy shows elongated serpentine telangiectasias with a whitish structureless background.29 Ulceration appears to be relatively frequent and has been
Involvement of the penis with lesions resembling chronic balanitis has been described.40–42 Exceptional involvement of the scrotum has also been described.43 Rarely, lesions are associated with Koebner phenomenon.44–46 Necrobiotic and silicotic granulomata developing within phlebectomy scars have also been reported.47 The condition may also occur in association with surgical scars after appendicectomy and breast reconstruction surgery, exceptionally at the site of a burn and in association with a tattoo.8,48–50
The disease tends to chronicity. It is of interest that necrobiosis lipoidica has been reported to be associated with cutaneous hypo- or complete anesthesia in both diabetic and nondiabetic patients.51,52 One study found loss of nerves within lesions and, based on this finding, the authors postulated that destruction of nerves might explain the sensory loss that is observed in some patients.52,53 Hypohidrosis and partial alopecia have also been reported.54
322 Granulomatous, necrobiotic and perforating dermatoses
It has been suggested that the lesions develop as a consequence of diabetic microangiopathy: the vessel walls in lesions of necrobiosis lipoidica are typically thickened by a diastase-resistant PAS-positive material. This does not explain the development of necrobiosis lipoidica in nondiabetic patients or the absence of the disease in patients with established microvascular lesions. An association with venous insufficiency and hypercholesterolemia has been suggested in a very small group of patients.64 The significance of this finding is therefore unclear. Study of microcirculation by Doppler flowmetry and oxygen partial pressure in necrobiosis lipoidica lesions in nondiabetics has demonstrated an altered microcirculation.65 Low oxygen and high carbon dioxide pressures, presumably reflecting ischemia, characterize necrobiotic plaques.66 Such vascular changes, although possibly causal, could equally well develop as a consequence of the necrobiotic changes. Aberrant platelet aggregation may also play a role in pathogenesis. Platelet survival times are markedly reduced in patients with necrobiosis lipoidica.67 Whether this is of pathogenic importance is uncertain.
Autoantibodies against cytoskeleton proteins have been observed in sera from patients with necrobiosis lipoidica. These autoantibodies (IgG antitroponin, antidesmin, antikeratin, anti-insulin, antitrinitrophenol, and IgA and IgM antikeratin) were found to be elevated in patients with necrobiosis lipoidica compared with diabetic patients without evidence of necrobiosis lipoidica.68 What role, if any, these autoantibodies play in the pathogenesis of necrobiosis lipoidica is unclear. Synthesis of collagen by fibroblasts cultured from lesions is decreased compared with fibroblasts from normal skin.69
Rarely, squamous carcinoma may arise in long-standing lesions.55–59 One such case developed in association with perforating necrobiosis lipoidica.60
Pathogenesis and histologic features The precise pathogenesis of necrobiosis lipoidica is unknown. Of primary importance is the temporal relationship between collagen degeneration and the inflammatory infiltrate.61 The close association of necrobiosis lipoidica and diabetes mellitus suggests a causal relationship, but the exact mechanism is uncertain. In the past, some 60% of patients with necrobiosis lipoidica were reported as having coexistent diabetes mellitus.2,4,62,63 However, its reported prevalence in diabetes is only of the order of 3/1000.61 Furthermore, a recent study has found that only a minority of patients with necrobiosis lipoidica have diabetes.11
Also of uncertain significance is the reported detection, by immunofluorescence, of immunoreactants (IgM and C3) in blood vessel walls in some cases of necrobiosis lipoidica.70,71 Epidermal dendritic S100-positive cells are increased in number.72 Whether this reflects an immunological aspect to the development of necrobiosis lipoidica has yet to be determined.
Glut-1 (the human erythrocyte glucose transporter) is expressed by the fibroblasts in areas of sclerotic collagen from biopsies of patients with necrobiosis lipoidica.73 This raises the possibility of an altered transport of glucose in the affected areas contributing to the histopathological features seen in this disease.
323 Necrobiosis lipoidica
Gli-1, the glioma-associated oncogene homologue, has been found to be expressed in a number of granulomatous skin disorders including necrobiosis lipoidica.74 The explanation for this is not clear, but it suggests that inhibitors of gli-1 may be used in the treatment of the disease.
Recently, spirochetal microorganisms, likely to be Borrelia, have been identified in lesions of necrobiosis lipoidica in patients from central Europe.75 The significance of this finding is unclear.
consist of eosinophilic, swollen or degenerate collagen, often appearing hyalinized with a surrounding infiltrate of variable numbers of lymphocytes and histiocytes (Fig. 9.57). Aggregates of lymphoid cells, with or without germinal center formation, are frequently found.78 Plasma cells are almost invariably present. In a single case, the plasma cell infiltrate was monoclonal, and further investigations revealed an underlying monoclonal gammopathy.79 The necrobiotic foci sometimes contain mucin. Palisading is variable, being more conspicuous in those instances associated with a heavy inflammatory cell infiltrate. The areas of necrobiosis are associated with loss of elastic tissue (Fig. 9.58). Usually, epithelioid histiocytes and giant cells are evident and sometimes there are well-formed granulomata resembling the sarcoidal type of necrobiotic histologic reaction (see below) (Fig. 9.59). Very rarely, asteroid bodies are identified.80 Lipid droplets, best seen with oil red O or Sudan IV staining on frozen tissue, are almost invariably present in the necrobiotic foci. Usually, a mild to moderate perivascular lymphocytic infiltrate is seen in the adjacent dermis. Cholesterol clefts are rare and only exceptionally may be prominent.81,82

Fig. 9.50 Necrobiosis lipoidica: characteristic, bilateral, symmetrical lesions. From the collection of the late N.P. Smith, MD, the Institute of Dermatology, London, UK.

Fig. 9.51 Necrobiosis lipoidica: typical lesion with an erythematous border. From the collection of the late N.P. Smith, MD, the Institute of Dermatology, London, UK.
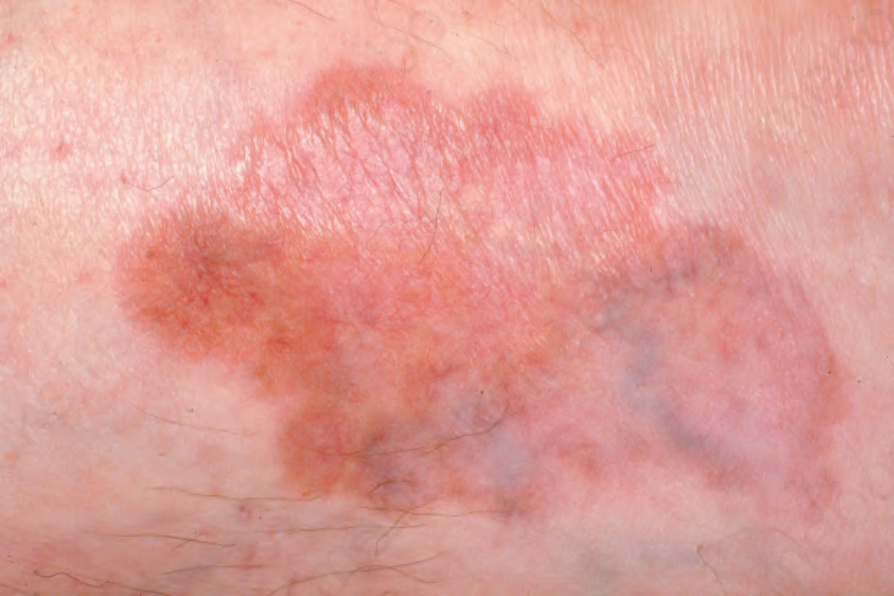
Fig. 9.52 Necrobiosis lipoidica: lesion on shin showing atrophy and telangiectasia. From the collection of the late N.P. Smith, MD, the Institute of Dermatology, London, UK.

Fig. 9.53 Necrobiosis lipoidica: chronic lesion with ulceration and crusting. From the collection of the late N.P. Smith, MD, the Institute of Dermatology, London, UK.
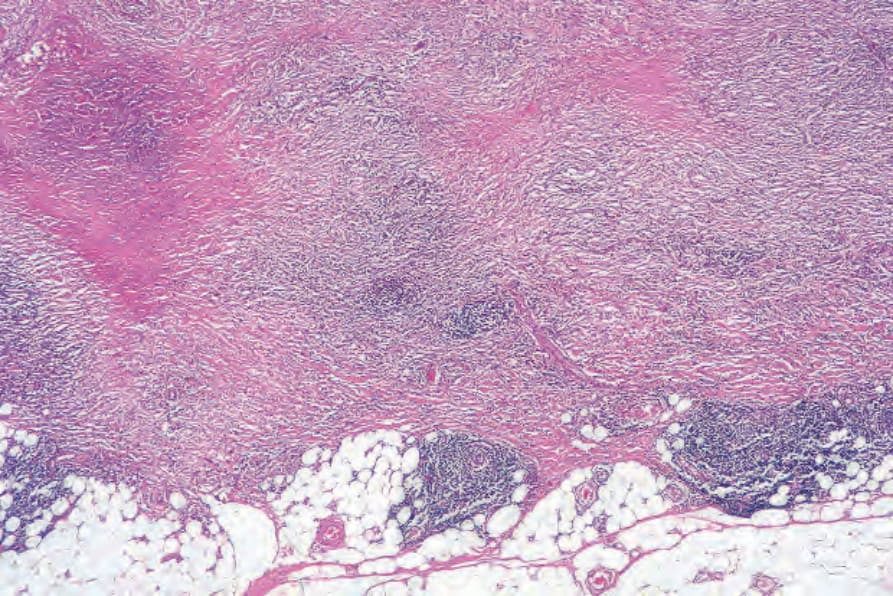
Fig. 9.55 Necrobiosis lipoidica: the lesion extends down to the subcutaneous fat.
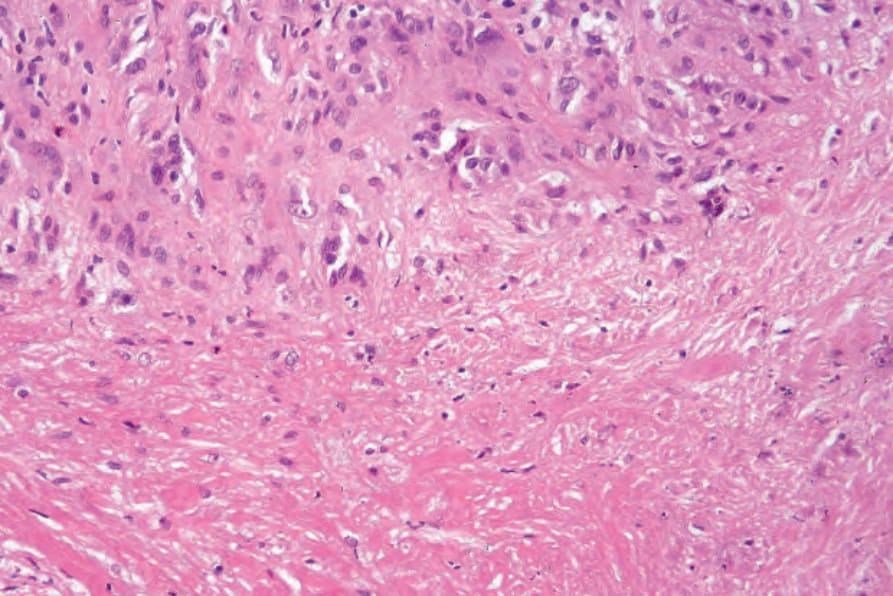
Fig. 9.56 Necrobiosis lipoidica: high-power view of Fig. 9.54.
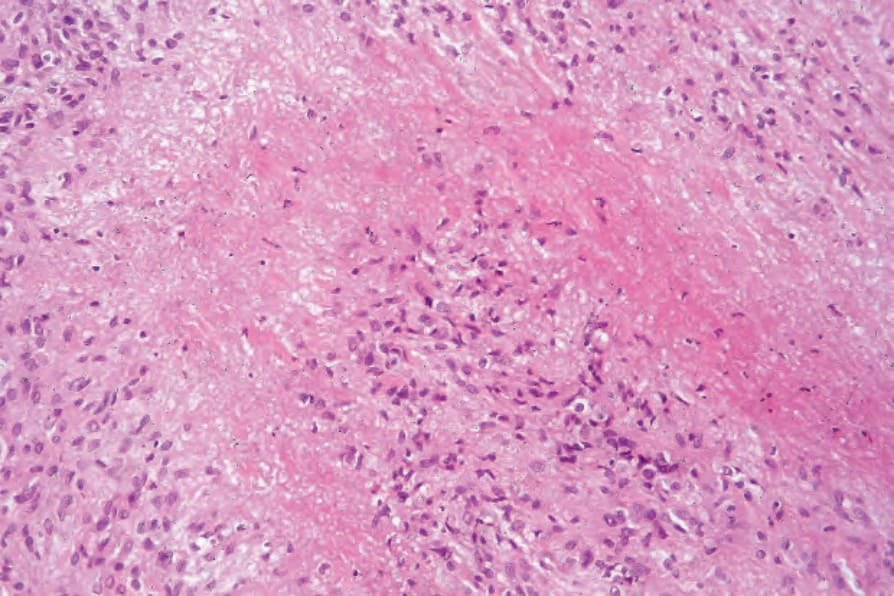
Fig. 9.57 Necrobiosis lipoidica: the degenerate collagen is surrounded by a palisade of histiocytes, lymphocytes, and fibroblasts.

Fig. 9.58 Necrobiosis lipoidica: note the complete absence of elastic tissue. Elastic-van Gieson.
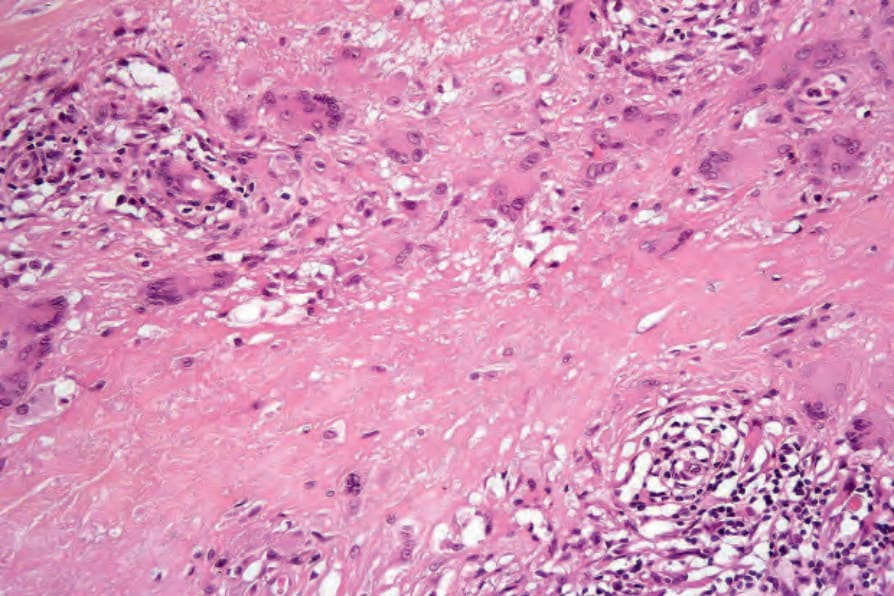
Fig. 9.59 Necrobiosis lipoidica: there is a granulomatous infiltrate with conspicuous multinucleate giant cells.
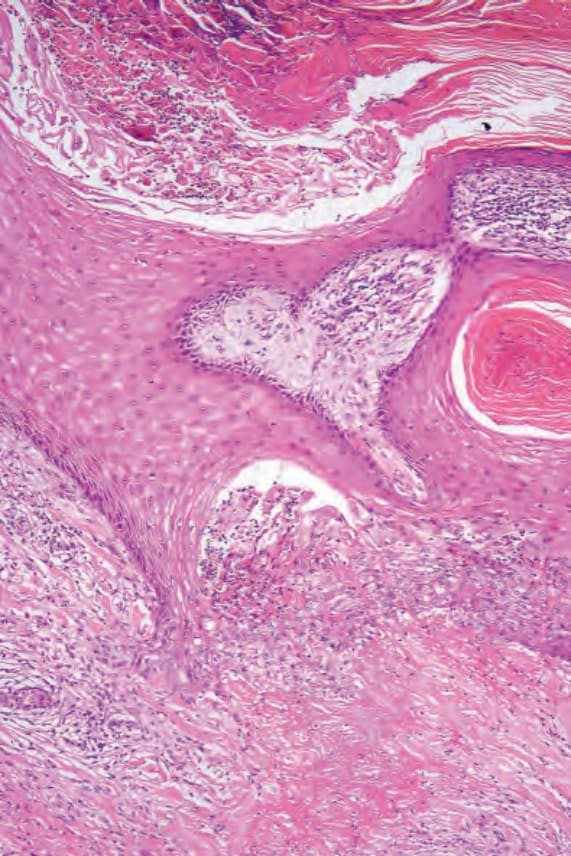
Fig. 9.65 Perforating necrobiosis: close-up view of the perforating channel.
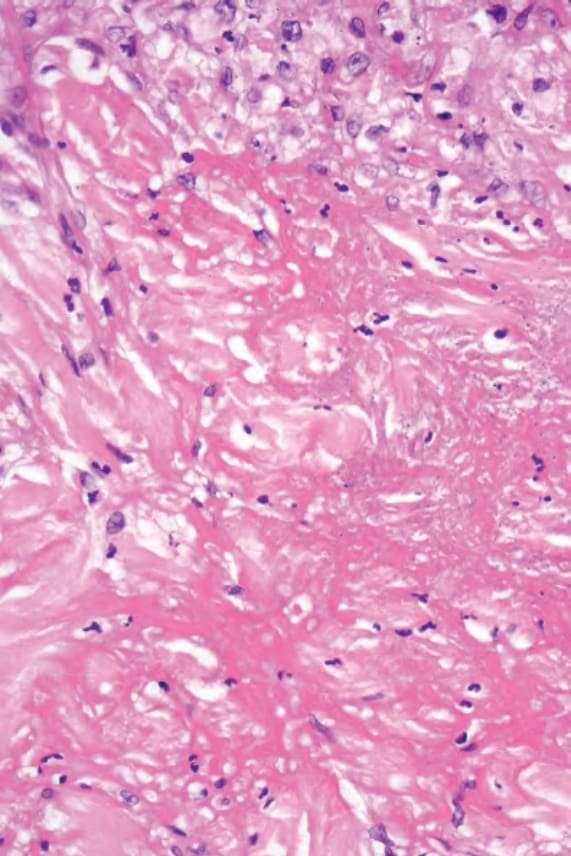
Fig. 9.66 Perforating necrobiosis: the dermis immediately beneath the site of perforation shows severe necrobiotic change.

Fig. 9.67 Rheumatoid nodules: lesions on the knuckles are commonly seen in rheumatoid arthritis. By courtesy of Dr J.C. Pascual, MD, Alicante, Spain.

Fig. 9.68 Rheumatoid nodule: close-up view. By courtesy of Dr J.C. Pascual, MD, Alicante, Spain.
The histopathological features are variable, depending to some extent on the presence or absence of coexistent diabetes mellitus.76,77 The palisading granuloma with necrobiosis is more typical of the diabetes-related variant, whereas a granulomatous sarcoidal type of reaction is more often a feature of nondiabetes-related necrobiosis. Nevertheless, there is very considerable overlap and in the majority of cases one cannot predict, on histologic grounds alone, which cases are, and which are not, diabetes-related.
The epidermal changes are usually inconspicuous or absent. There may, however, be acanthosis or atrophy, and hyperkeratosis is not uncommon.
The hallmark of necrobiosis lipoidica is the palisading necrobiotic granuloma. Large, often confluent areas of necrobiosis are present, usually centered in the lower dermis, although the superficial dermis and subcutaneous fat may also be affected (Figs 9.54–9.56). When the subcutaneous fat is involved, the changes are seen mainly in the septa. The foci of necrobiosis
A careful search often reveals vascular changes in necrobiosis lipoidica. These consist of blood vessel wall thickening, with intimal proliferation and narrowing of the lumen. Occasionally, thrombi are noted. Sometimes increased numbers of vessels are a feature. The vascular changes are more obvious in patients with associated diabetes mellitus or other systemic disease. These changes are particularly severe in those cases where
324 Granulomatous, necrobiotic and perforating dermatoses
necrobiosis is very marked. One study also showed that neutrophilic and granulomatous vasculopathies correlated with systemic disease.83 In addition, telangiectatic superficial venules are a common feature. Cases with necrobiosis-like features and significant vasculitis and neutrophilic infiltrates in the setting of systemic disease are discussed in detail in the section on palisaded neutrophilic and granulomatous dermatitis associated with systemic disease (p. 334). In lesions with anesthesia, S100 shows destruction of nerve fibers in the areas of necrobiosis.52,53
In the diffuse variant, there is very widespread necrobiosis with a minimal inflammatory cell response; such cases are usually associated with diabetes (Fig. 9.60). Sometimes linear infiltrates of histiocytes between collagen fibers are a feature, as in granuloma annulare. Lipomembranous fat necrosis is noted in occasional cases.84
In the sarcoidal type of necrobiosis lipoidica, which is more often noted with the nondiabetes mellitus-associated variant, the appearances are those of naked epithelioid cell granulomata, particularly in the lower dermis (Fig. 9.61). Langhans and foreign body giant cells are usually conspicuous, and a lymphocytic and plasma cell infiltrate may be evident (Fig. 9.62). Necrobiosis is usually minimal; multiple levels may have to be examined before its presence is confirmed (Fig. 9.63). The sarcoidal type of necrobiosis lipoidica in patients without diabetes mellitus has in the past been described as Miescher granuloma.
Perforating necrobiosis lipoidica is associated with transepidermal elimination of necrobiotic collagen and also degenerated elastotic material (Figs 9.64–9.66).81,85,86
Exceptionally, skin changes at the sites of intravenous drug abuse and leishmaniasis may mimic necrobiosis lipoidica.87,88 Histologic changes of both necrobiosis lipoidica and granuloma annulare may exceptionally coexist in a tattoo reaction.89 A small number of patients reported in a series presented with pretibial lesions suggestive of necrobiosis lipoidica, but on histology, only features of venous insufficiency were observed. The name of pretibial angioplasia has been proposed for this entity.90
Differential diagnosis Necrobiosis lipoidica must be distinguished from granuloma annulare, rheumatoid nodule, actinic granuloma, and granuloma multiforme. Points of
325 Necrobiosis lipoidica
distinction are summarized in Table 9.1. The presence of massive necrobiosis associated with numerous cholesterol clefts, bizarre multinucleated giant cells, and Touton-type giant cells distinguishes necrobiotic xanthogranuloma from necrobiosis lipoidica. As noted above, prominent cholesterol cleft formation, which is a feature that usually suggests necrobiotic xanthogranuloma, may rarely be seen in necrobiosis lipoidica.76,77 Small punch biopsies may not be adequate for definitive evaluation, and sampling bias may be misleading. Clinical correlation should be taken into consideration before making a final diagnosis. It has been proposed that the pattern of immunostaining with adipophilin may be of use in the differential diagnosis of granulomatous dermatitis. In necrobiosis lipoidica adipophilin staining is usually limited to extracellular areas in zones of damaged collagen, whereas in granuloma annulare there is extracellular and intracellular staining and in sarcoidosis the staining tends to be intracellular.91
326 Granulomatous, necrobiotic and perforating dermatoses
Lesions are often fixed to the underlying periosteum or deep fascia. They present as firm, asymptomatic, dome-shaped masses in the subcutaneous fat or deeper tissues and measure from several millimeters to 5 cm in diameter. Numbers may vary from one to over a hundred. Ulceration sometimes occurs. Intrapulmonary rheumatoid nodules have been exceptionally associated with leflunomide in a patient with rheumatoid arthritis.15 A rare association with anti-tumor necrosis factor alpha treatment for rheumatoid arthritis has been described.16 A case of large cavitary pulmonary lesions in a patient with HIV has been reported.17
Rheumatoid nodules are more commonly found in patients with severe rheumatoid arthritis and are associated with a high titer of rheumatoid factor, joint erosions, and an increased incidence of rheumatoid vasculitis.18 They are not, however, specific for rheumatoid arthritis, being found in approximately 5–7% of patients with SLE (although in this condition they tend to be localized about the hands) and occasionally in seronegative ankylosing spondylitis.19,20 Clinically similar lesions have also been reported in patients with scleroderma. Presentation of multiple rheumatoid nodules on the fingers in association with little or no arthritis has been described as rheumatoid nodulosis.21–23 This, however, can be associated with destructive arthritis.24 A similar name (cutaneous nodulosis) has been given to the development of multiple small nodules at different sites during methotrexate therapy for rheumatoid arthritis.25 Etanercept has been linked to the exceptional development of extensive pulmonary nodulosis, while infliximab and the aromatase inhibitor letrozole are associated with accelerated cutaneous nodulosis.26–28
Pathogenesis and histologic features Although these lesions develop at sites of pressure and trauma (implying pathogenetic significance), there is some evidence in support of an immune complex-mediated pathogenesis, as both IgG and IgM have been detected by immunofluorescence in the walls of blood vessels adjacent to rheumatoid nodules.29 Similarly, both rheumatoid factor and complement have been demonstrated within the substance of rheumatoid nodules. Localization of IgM rheumatoid factor and terminal complement complexes C5b-9 has been demonstrated on the luminal surface of endothelial cells in rheumatoid nodules.30 C4d has been shown in association with palisading macrophages and in areas of fibrinoid necrosis, further supporting the role of complement activation in the pathogenesis of the lesions.31 Proinflammatory cytokines and cell adhesion molecules (TNF-α, IL-1β, IL-Ra RNA, E-selectin) have been shown in rheumatoid nodules and are likely to play a role in mediating injury.32 The expression of cytokines in the rheumatoid nodule is very similar to that in the synovial lining in rheumatoid joints and suggests that the pathogenesis of both is very similar and driven by Th1 lymphocytes.33 The cytokines involved include IFN-γ, IL-1beta, TNF-α, IL-12, IL-18, IL-15,
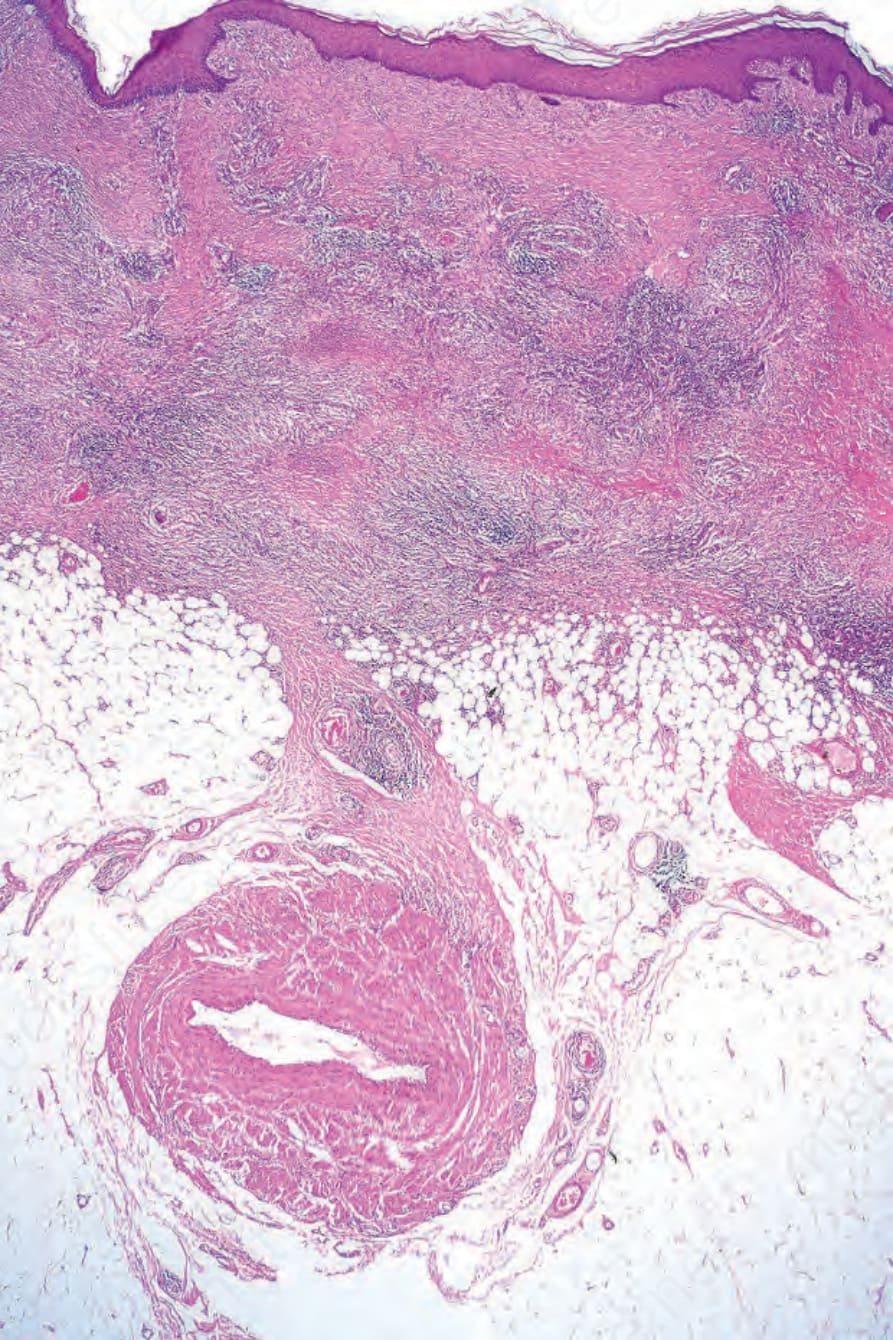
Fig. 9.54 Necrobiosis lipoidica: the epidermis is unaffected; there is extensive necrobiosis in the reticular dermis. A heavy chronic inflammatory cell infiltrate is present.
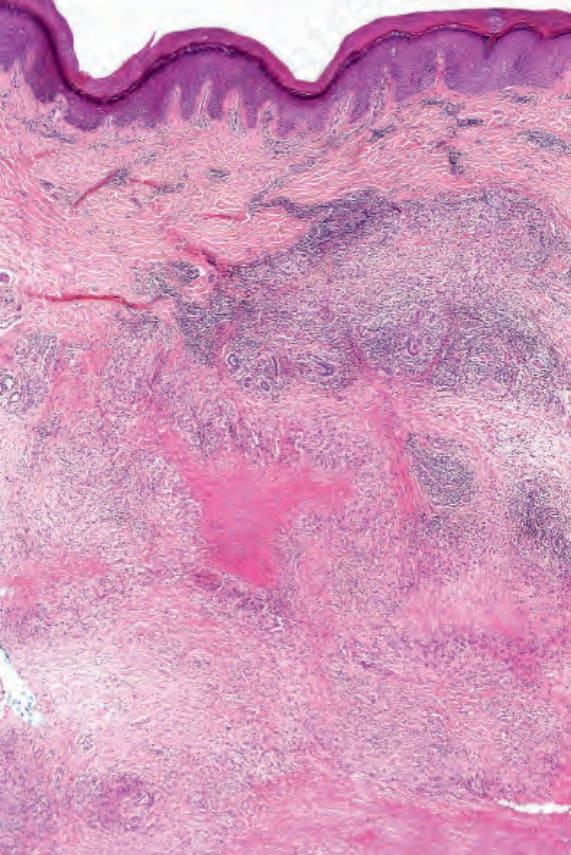
Fig. 9.60 Necrobiosis lipoidica (diffuse variant): a broad band of confluent necrobiosis has destroyed the entire reticular dermis.
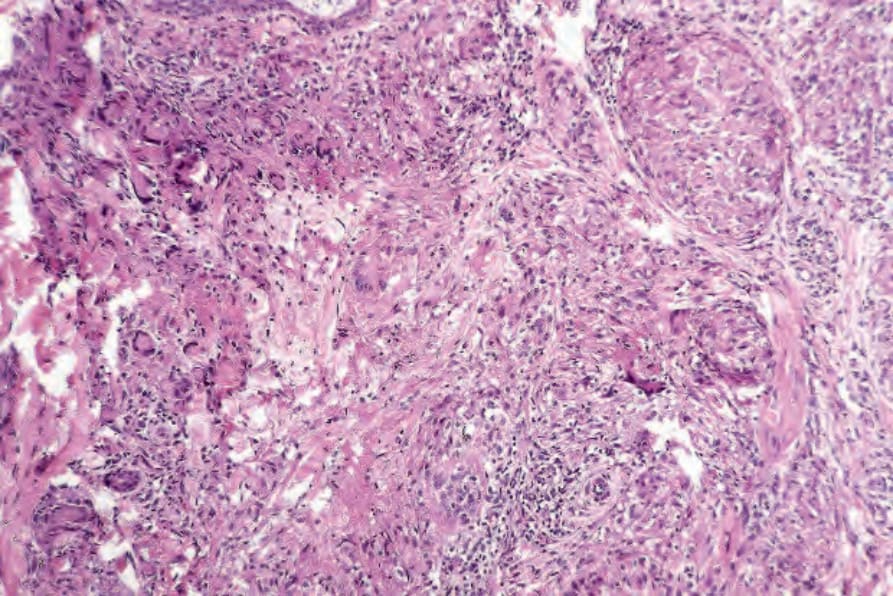
Fig. 9.61 Necrobiosis lipoidica (granulomatous variant): well-defined noncaseating granulomata replace the reticular dermis. Necrobiosis is present to the left of center.
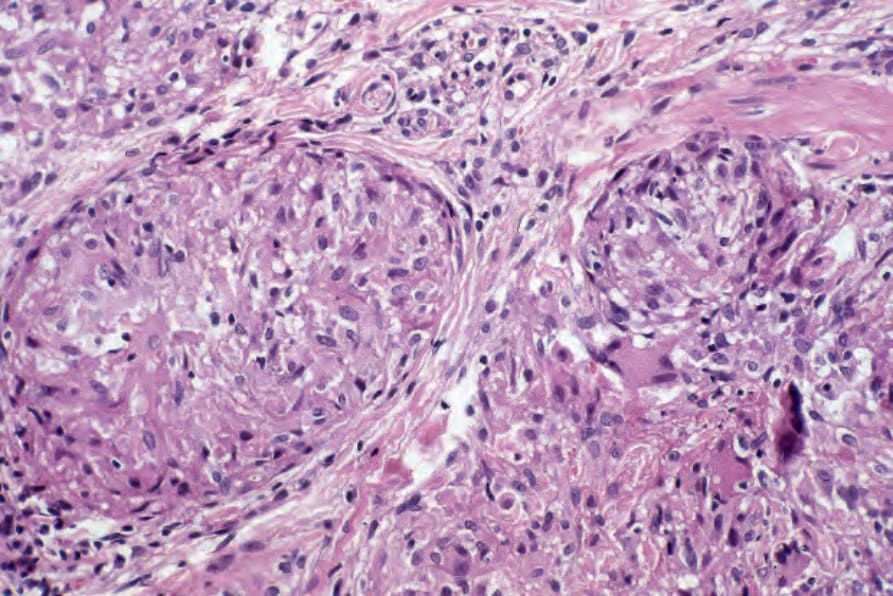
Fig. 9.62 Necrobiosis lipoidica (granulomatous variant): the naked granulomata are very reminiscent of sarcoidosis. Note the multinucleate giant cells.
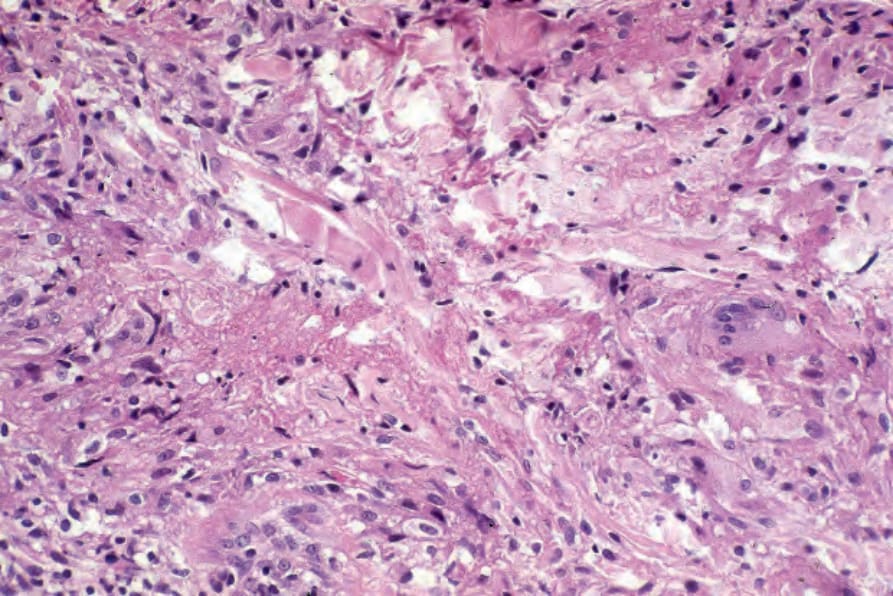
Fig. 9.63 Necrobiosis lipoidica (granulomatous variant): higher-power view of the necrobiotic focus seen in Fig. 9.61.
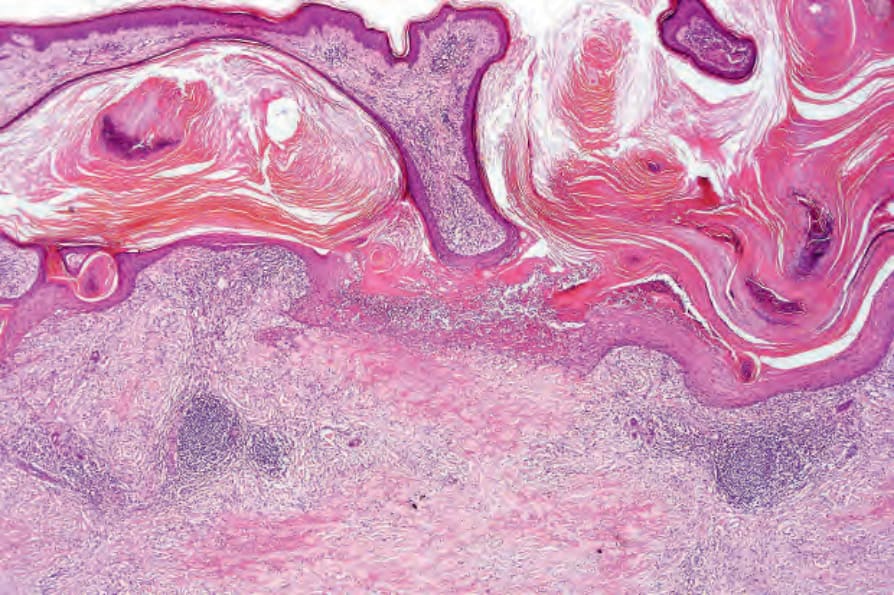
Fig. 9.64 Perforating necrobiosis lipoidica: there is widespread hyperkeratosis and crusting. A perforating channel is seen on the right side of the picture.
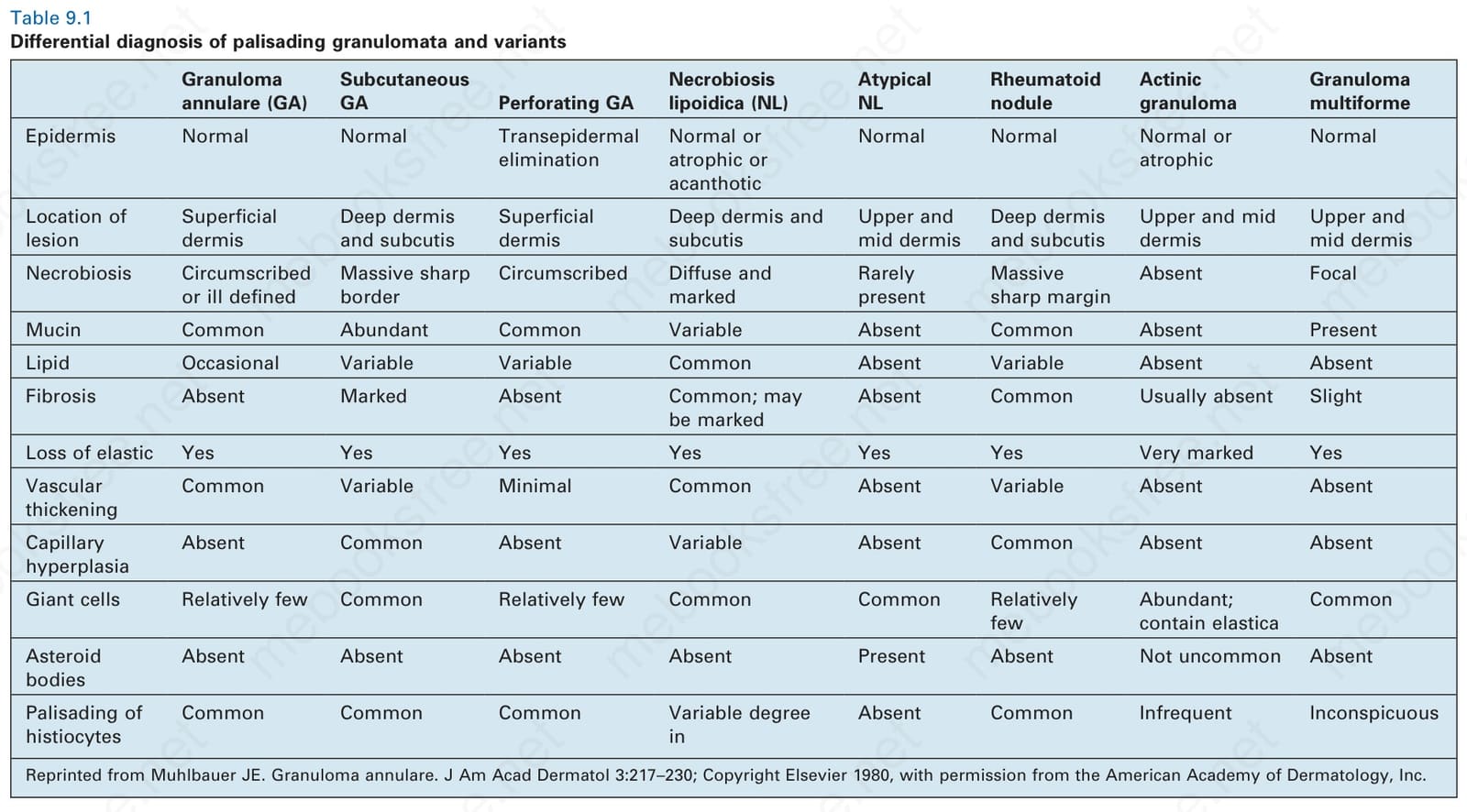
Table 9.1 Differential diagnosis of palisading granulomata and variants