Pregnancy prurigo
Pregnancy prurigo
Clinical features Pregnancy prurigo (prurigo gravidarum, prurigo gestationis) has recently been classified under the broader disease group atopic eruption of pregnancy.1,2 It affects 1 in 300 pregnancies, presenting as pruritic, erythematous, 0.5–1.0-cm papules and nodules with a predilection for the extensor surfaces of the extremities and the abdomen.1,3–9 Superimposed features of excoriation with scale-crust may be seen. Lesions usually present during the third trimester, but may present at all stages of pregnancy.1 The condition usually disappears following delivery, but in some cases, it persists into the puerperium. Blistering is not a feature. Fetal and maternal health does not appear to be adversely affected.7
Pathogenesis and histologic features The pathogenesis of pregnancy prurigo is unknown. It has been suggested that the condition represents pruritus gravidarum in a background of atopic dermatitis.3,7 Patients often have a history of atopy.7 Serum IgE may be elevated in patients regardless of whether or not there is a positive history of atopy.7 Of interest, eczematous dermatitis appears to be common in pregnancy.7 Furthermore, a comprehensive analysis of dermatoses of pregnancy suggested that there is significant clinical and histologic overlap between eczema of pregnancy, pruritic folliculitis of pregnancy, and prurigo of pregnancy and that they should be regarded as a single disease complex termed ‘atopic eruption of pregnancy’.1
The histologic features are not specific, comprising mild spongiosis, lymphocytic exocytosis, and a superficial perivascular lymphohistiocytic infiltrate with occasional eosinophils (Figs 8.56 and 8.57).10 Frequently, histologic features of excoriation are present. Immunofluorescence studies are negative.
Differential diagnosis The histologic features are non-specific and clinical correlation is necessary to render a firm diagnosis. The diagnosis is perhaps best approached as one of exclusion, and underlying etiologies should be sought. The major differential diagnosis includes hypersensitivity reactions (drug eruption, insect bites, etc.) with superimposed prurigo nodularis.
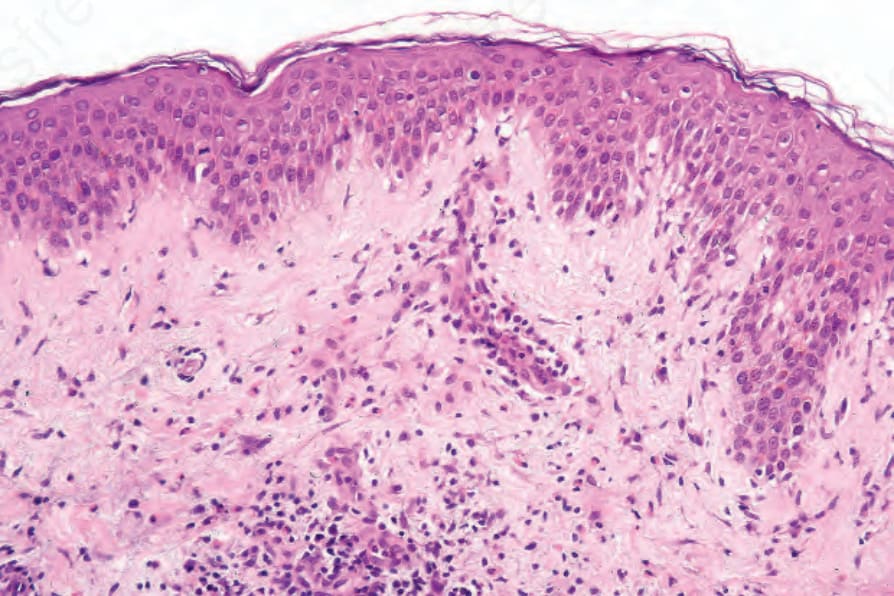
Fig. 8.56 Pregnancy prurigo: there is a superficial perivascular inflammatory cell infiltrate.
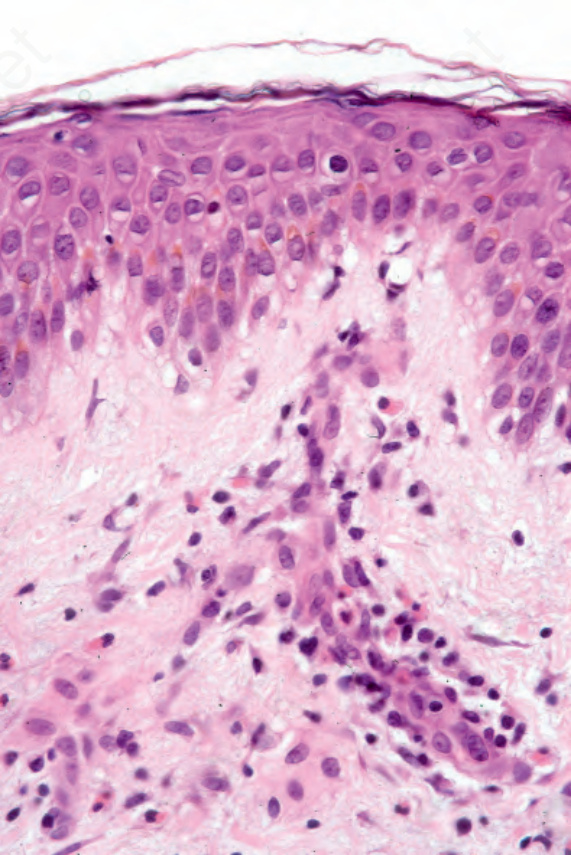
Fig. 8.57 Pregnancy prurigo: the infiltrate consists of lymphocytes with occasional eosinophils.