Lichen aureus
Lichen aureus
Clinical features Lichen aureus (lichen purpuricus) is a rare variant of the pigmented purpuric dermatoses. It may be differentiated from the other forms by virtue of its distinctive clinical and histologic features.1–4 It is, therefore, discussed separately.
Lichen aureus shows a male predilection (2 : 1) and tends to affect the younger age group, with a peak incidence in the fourth decade. Children may occasionally be affected.3 Lesions are usually asymptomatic, although pruritus is an occasional feature. The disease is characterized by discrete or confluent lichenoid macules and papules, which may be golden yellow, bronze, purple, or dark brown, and may resemble a bruise (Fig. 8.50). Sometimes a purpuric element is evident. The lesions of lichen aureus are characteristically very persistent, although occasionally spontaneous resolution is a feature. They occur most often on the lower legs, but may affect quite a wide variety of sites, including the arms, hands, trunk, thighs, and vulva.5–8 Lesions are usually unilateral and limited to only one or two sites; they consist of either solitary ovoid maculopapules 3–5 cm in diameter or irregular plaques up to 20 cm across. Rarely, a zosteriform, segmental or agminate distribution, has been described.8–11
In one study, a monoclonal T-cell population was observed in 50% of the cases studied. No progression to mycosis fungoides was seen in these cases.7
Differential diagnosis There may be some histologic overlap with the Gougerot-Blum variant of pigmented purpuric lichenoid dermatitis, but lichen aureus tends to be more localized.
Histologic features The epidermis is structurally normal. A dense lymphohistiocytic infiltrate is present in the upper dermis, usually distributed in a bandlike fashion immediately below the epidermis (Figs 8.51 and 8.52). In contrast to lichen planus, however, there is no evidence of basal cell hydropic degeneration and cytoid bodies are not usually found. A Grenz zone is sometimes present, although the infiltrate may abut the overlying epidermis. Lymphocytic exocytosis is sometimes present. Scattered within the infiltrate are increased numbers of blood vessels. Hemosiderin-laden macrophages are present in the deeper aspect of the infiltrate or in the adjacent noninfiltrated dermis. Purpura is a variable feature and there is no evidence of frank vasculitis.

Fig. 8.50 Lichen aureus: golden-red-brown plaques on the ankle. By courtesy of M. Price, MD, St Thomas’ Hospital, London, UK.
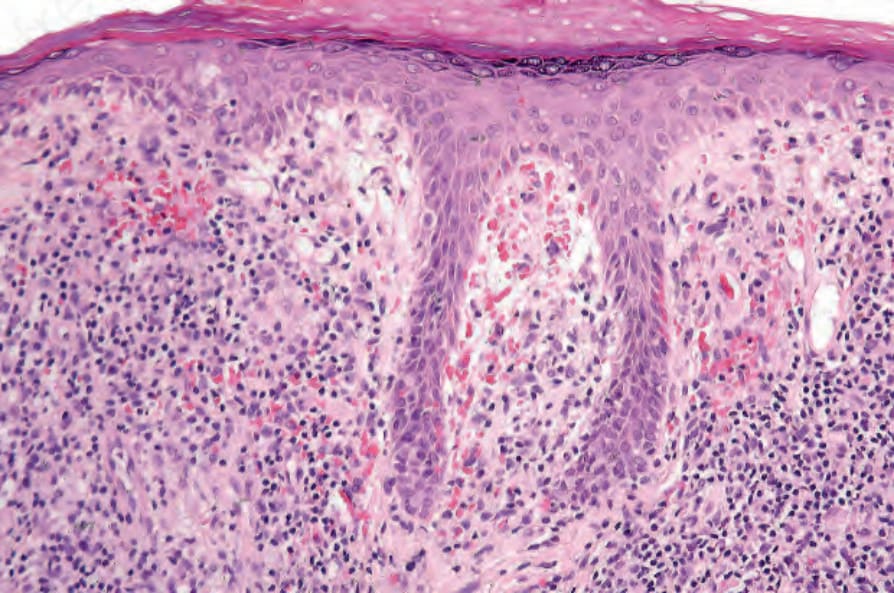
Fig. 8.51 Lichen aureus: there is a dense bandlike infiltrate in the upper dermis.
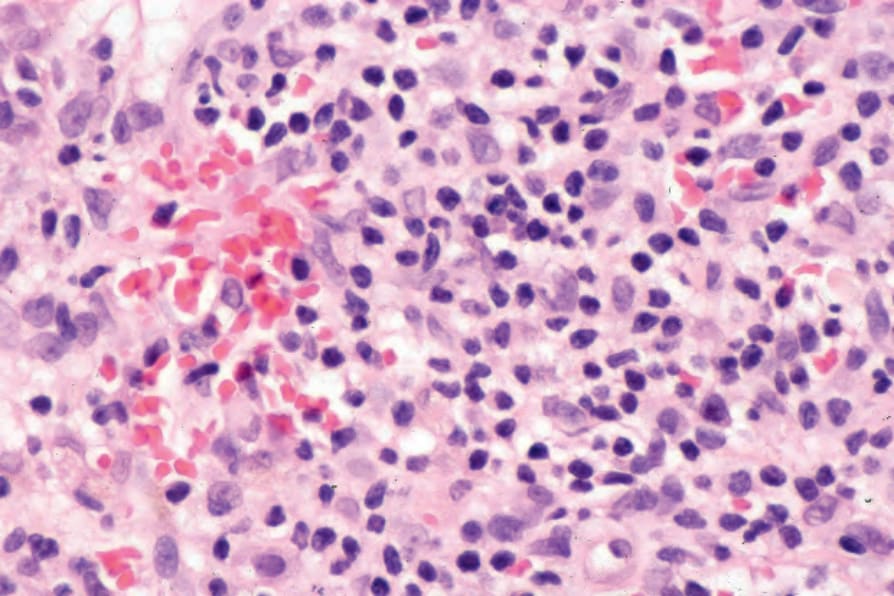
Fig. 8.52 Lichen aureus: the infiltrate consists of lymphocytes and histiocytes. Note the marked red cell extravasation.