Pityriasis lichenoides
Pityriasis lichenoides
Clinical features Pityriasis lichenoides (Gr. pityron, bran + iasis; lichen; Gr. eidos, form) is an uncommon dermatosis of unknown etiology, although a hypersensitivity reaction to a number of infectious agents including adenovirus, toxoplasmosis, Epstein-Barr virus, and Mycobacterium pneumoniae have been
279 Interface dermatoses
proposed.1–4 The condition has also been documented in association with a range of autoimmune conditions such as rheumatoid arthritis, hypothyroidism, and pernicious anemia.3,4 Two cases of pityriasis lichenoides chronica (PLC) associated with adalimumab therapy for Crohn disease and cases induced by infliximab have been described.5,6,7 The term includes a spectrum of disease manifestations, ranging from the acute ulceronecrotic lesions of pityriasis lichenoides et varioliformis acuta (PLEVA, also known as Mucha-Habermann disease or acute guttate parapsoriasis) to the more chronic scaly papules of PLC (chronic guttate parapsoriasis); there is often clinical overlap.8–13 In addition, a febrile, ulceronecrotic variant (febrile ulceronecrotic Mucha-Habermann disease) is recognized.3–9,13
Pityriasis lichenoides in more recent studies lacks strong sex predominance in adults. However, some studies have shown more of a male predominance in pediatric populations.12,14–16 It most often occurs in childhood (5–10 years of age) and early adulthood, second or third decade.12–16
Lesions show a propensity to involve the arms, legs, trunk, and buttocks (Fig. 7.122). The upper limbs appear to be involved more often than the lower and the flexor more commonly than the extensor surfaces. They can begin as small macules that progress to papules. PLC is typically asymptomatic while PLEVA is associated with burning and pruritus.10,13 The onset is usually insidious and the course fluctuating and episodic, patients experiencing recurrent crops of lesions, with the exception of the ulceronecrotic variant which is rapid. Duration of the rash is quite variable: although many patients are free of lesions by 3–6 months, others show great persistence of the disease, often for many years.12,13 The disease shows some seasonal variation, with lesions worsening in winter and showing improvement in sunlight. Although pityriasis lichenoides is traditionally divided into acute and chronic variants, not uncommonly both types of lesions can be seen in the same patient, indicating a possible connection between PLC and PLEVA.10
In the more acute form of the disease, the initial lesions are crops of pink papules (Figs 7.123 and 7.124). These may become vesicular or hemorrhagic and ultimately develop necrosis and ulceration (Fig. 7.125). Healing is usually associated with the development of superficial varioliform scars. Postinflammatory hyper- or hypopigmentation is not uncommon (Fig. 7.126).10,12,13 The rash is often polymorphic, individual patients having lesions at varying stages of evolution. Patients may be pyrexic and sometimes lymphadenopathy is present.1
The chronic lesions are typified by numerous, lichenoid, brownish-red, scaly papules, 3–10 mm across, the scale being most noticeable peripherally, sometimes referred to as the mica scale (Figs 7.127 and 7.128). These lesions usually heal without scarring, but are sometimes associated with hypopigmentation, which may be the most prominent feature in dark-skinned races.
Although there are case reports of lymphoma (mycosis fungoides) developing in patients with pityriasis lichenoides, this is a rare event (see also below).16–20
The rare febrile ulceronecrotic variant is associated systemic features including fever, muscle weakness and pain, malaise, lymphadenopathy, arthritis, myocardial involvement, neuropsychiatric manifestations, pulmonary involvement, and even death.3–9,12,13,21–26 Widespread cutaneous manifestations include large 2–6-cm ulceronecrotic lesions, hemorrhagic and necrotic papules, and erythema multiforme-like lesions.3,4,12,13,21–26
Pathogenesis and histologic features Immunofluorescence examination of biopsies from fresh purpuric lesions commonly detects IgM and C3 in the walls of the superficial dermal blood
280 Lichenoid and interface dermatitis
A
B
vessels and along the dermal–epidermal junction in both the acute and chronic forms of the disease, though this is not used diagnostically.27–29 A high proportion of patients have elevated circulating immune complexes.30,31 Cytotoxic suppressor T cells constitute the majority of the infiltrate in pityriasis lichenoides et varioliformis acuta.32,33 Lesser numbers are seen in PLC. These (and the overlying keratinocytes in addition to nearby endothelial cells) have been shown to express HLA-DR.33 In contrast to lymphomatoid papulosis, CD30 is generally not expressed in pityriasis lichenoides acuta except in what has been described as overlap cases.34,35 It is however, unlikely that the two conditions truly overlap. Macrophages are also numerous. Langerhans cells are diminished in number. Clonal T-cell receptor gene rearrangements have been described in small numbers of patients with pityriasis lichenoides acuta leading to the suggestion of a possible overlap with cutaneous T-cell lymphoma.36,37 Exceptionally, pityriasis lichenoides acuta has been reported to progress to cutaneous T-cell lymphoma.12,13,18–20,38,39 As a result, some have suggested that PLEVA may represent a host response to a developing T-cell lymphoproliferative disorder in
281 Interface dermatoses
some cases.12 Complicating this issue are pityriasis lichenoides-like variants of mycosis fungoides.40–42
The histopathological features of pityriasis lichenoides are similar in both variants, although in the acute form the changes are usually more severe. Both are characterized by varying proportions of epidermal and dermal changes.13,43–46
The chronic lesions of pityriasis lichenoides are characterized by parakeratosis in which there are sometimes small collections of lymphocytes reminiscent of the Munro microabscesses of psoriasis (Figs 7.129 and 7.130). The epidermis may show slight acanthosis and usually small numbers of necrotic keratinocytes are present accompanied by multifocal but subtle interface change (Fig. 7.131). Spongiosis is often a feature. There is a perivascular, often wedge-shaped chronic inflammatory cell infiltrate in the superficial dermis (Fig. 7.132). Red cell extravasation is often present but is usually not marked.
The acute lesions of pityriasis lichenoides show similar epidermal features, but on a much exaggerated scale. Marked inter- and intracellular edema accompanied by keratinocyte necrosis and interface change frequently
282 Lichenoid and interface dermatitis
result in vesiculation and ulceration (Figs 7.133 and 7.134). Exocytosis is usually prominent and intraepidermal red blood cells are characteristic. The upper dermis is edematous and contains a chronic inflammatory cell infiltrate (Fig. 7.135). This is usually perivascular and varies from sparse to dense; typically, it has a wedge-shaped appearance, extending deeply into the reticular dermis, although this is only seen in biopsies from established lesions. The infiltrate consists of lymphocytes with an admixture of histiocytes. Red cell extravasation is usually conspicuous. The blood vessels of the superficial dermis are dilated and congested. Although the endothelial cells are often blurred or swollen, fibrinoid necrosis indicating necrotizing vasculitis is rarely seen (Fig. 7.136). The latter, if present is associated with lymphocytes and seen at the tip of the wedge in the mid to deep dermis. In febrile ulceronecrotic Mucha-Habermann disease, the features are those of very severe pityriasis lichenoides acuta and are often accompanied by changes of leukocytoclastic vasculitis.12,13,25,47
Differential diagnosis The differential diagnosis includes other interface dermatitides. In lichen planus, the infiltrate is bandlike rather than wedge shaped, the epidermis lacks parakeratosis, and hemorrhage is absent. In the erythema multiforme spectrum, hemorrhage is usually not prominent, the infiltrate is less dense, and the epidermis has a normal basket weave appearance. Lupus erythematosus lacks hemorrhage and has increased dermal mucin. Lymphomatoid papulosis can have both clinical and histologic overlap with PLEVA, but has large atypical CD30+ lymphocytes. Prior reports of patients having PLEVA and lymphomatoid papulosis likely represent lymphomatoid papulosis rather than a combination.2
Access ExpertConsult.com for the complete list of references

Fig. 7.122 Pityriasis lichenoides acuta: erythematous papules and crusted lesions are present on the buttocks and thighs. In severe cases, lesions may be very extensive. By courtesy of the Institute of Dermatology, London, UK.

Fig. 7.123 Pityriasis lichenoides acuta: typical lesions with pustulation are present on the arm, a commonly affected site. By courtesy of the Institute of Dermatology, London, UK.

Fig. 7.124 Pityriasis lichenoides acuta: early lesions are erythematous and papular. By courtesy of the Institute of Dermatology, London, UK.

Fig. 7.125 Pityriasis lichenoides acuta: (A) necrotic and ulcerated lesions are present; (B) close-up view. By courtesy of the Institute of Dermatology, London, UK.
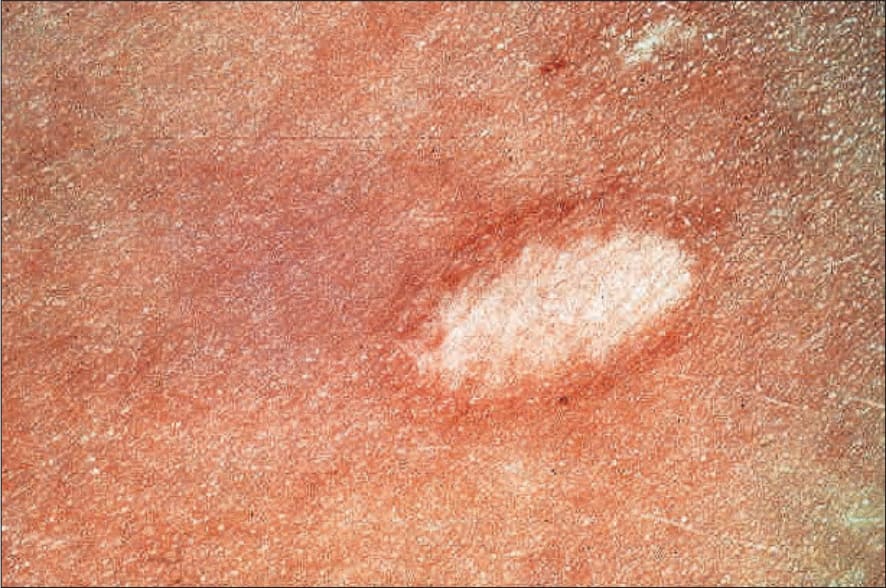
Fig. 7.126 Pityriasis lichenoides acuta: healed lesion showing scarring and hypopigmentation. By courtesy of the Institute of Dermatology, London, UK.

Fig. 7.127 Pityriasis lichenoides chronica: widespread scaly papules are present on the chest and arms. From the collection of the late N.P. Smith, MD, the Institute of Dermatology, London, UK.

Fig. 7.128 Pityriasis lichenoides chronica: the characteristic mica scale. By courtesy of the Institute of Dermatology, London, UK.

Fig. 7.129 Pityriasis lichenoides chronica: scanning view showing hyperkeratosis with parakeratosis and acanthosis.
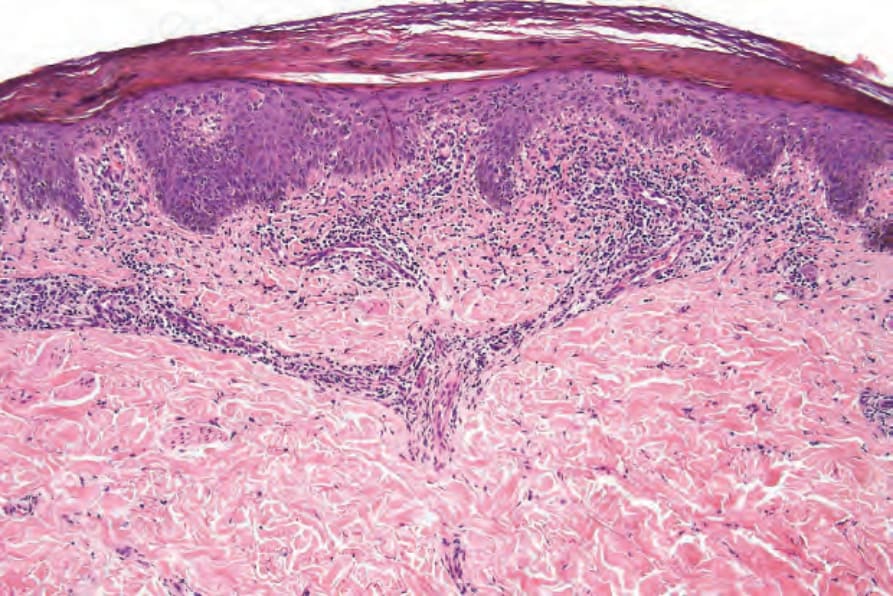
Fig. 7.130 Pityriasis lichenoides chronica: note the parakeratosis, acanthosis, and perivascular and interstitial chronic inflammatory cell infiltrate.
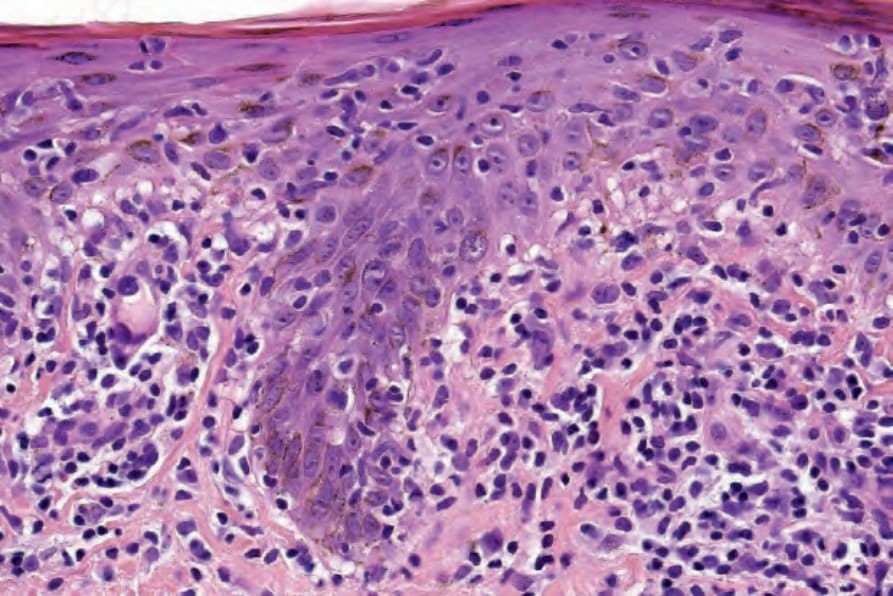
Fig. 7.131 Pityriasis lichenoides chronica: high-power view showing basal cell hydropic degeneration.
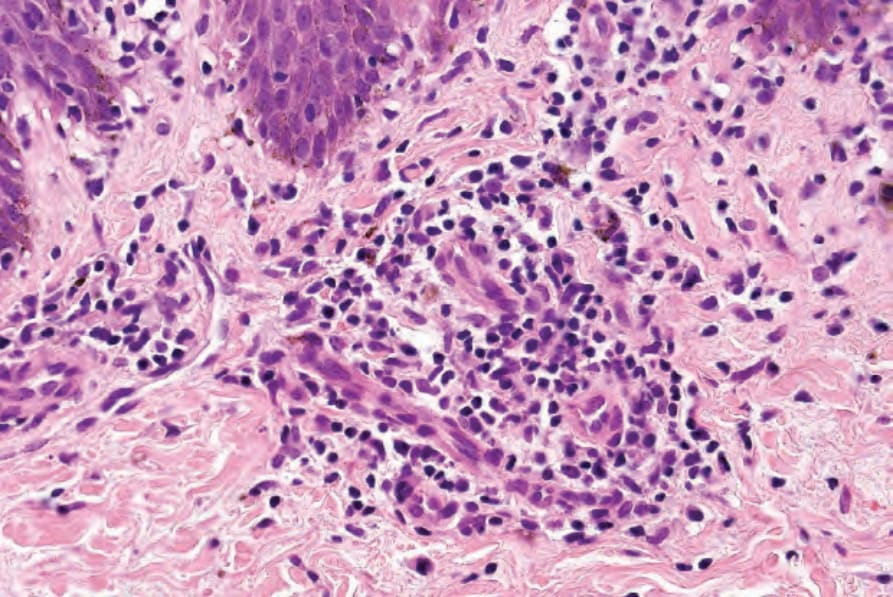
Fig. 7.132 Pityriasis lichenoides chronica: in this high-power view there is a lymphohistiocytic infiltrate and melanophages are present.
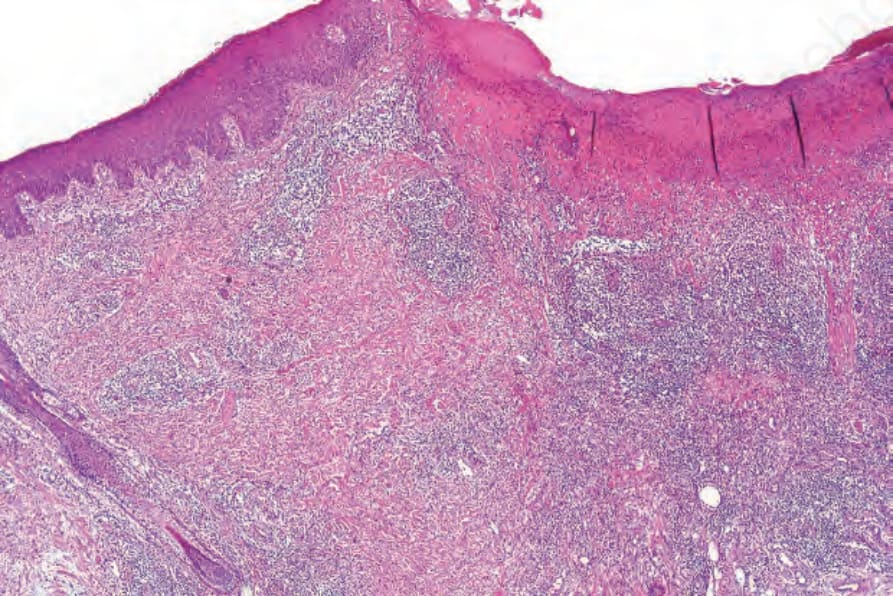
Fig. 7.133 Pityriasis lichenoides acuta: this low-power view shows an ulcerated papule with overlying crust.
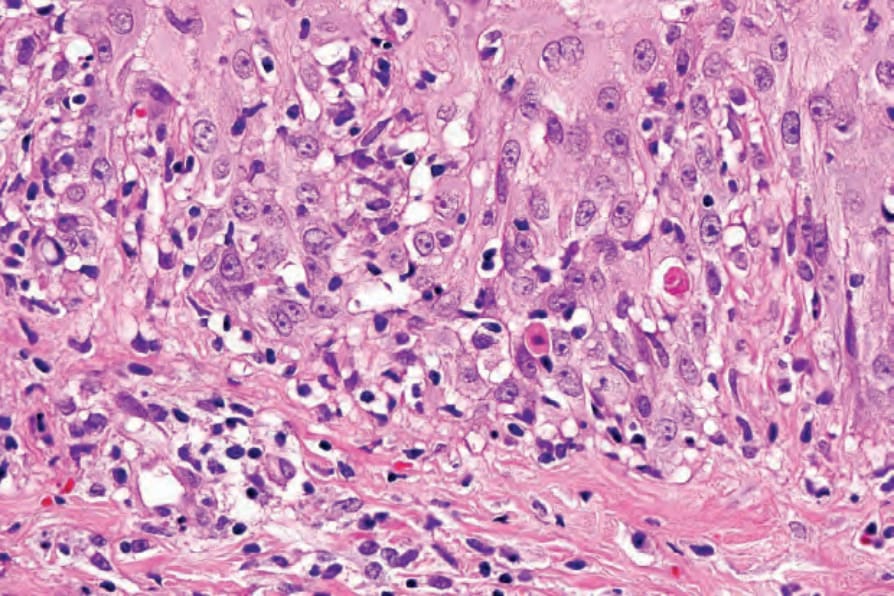
Fig. 7.134 Pityriasis lichenoides acuta: there is basal cell hydropic degeneration and apoptosis.
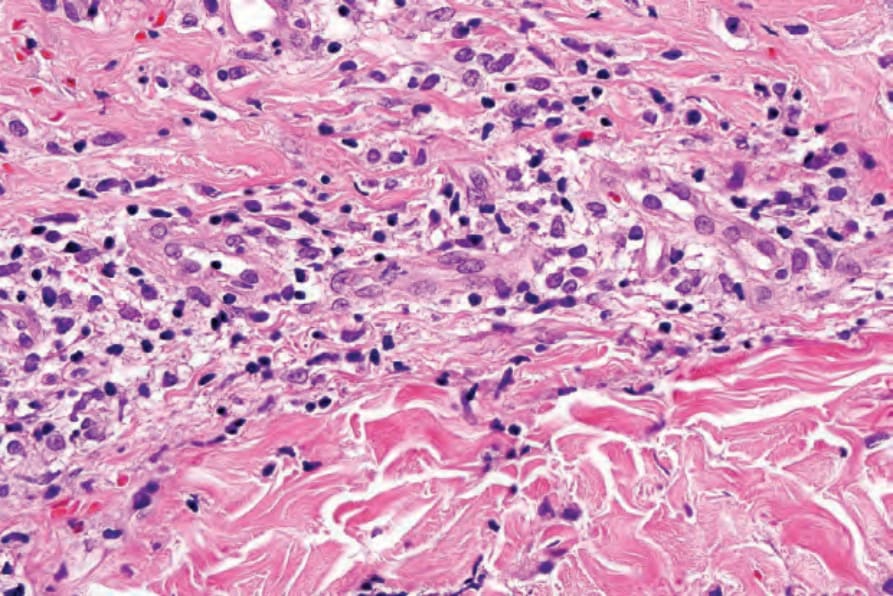
Fig. 7.135 Pityriasis lichenoides acuta: this high-power view shows a lymphohistiocytic infiltrate. Red cell extravasation can also be seen.
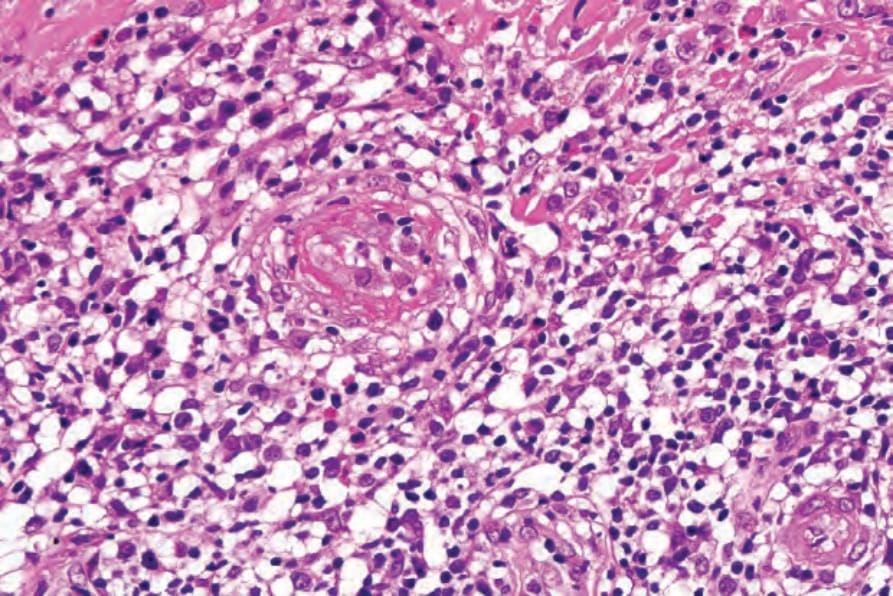
Fig. 7.136 Pityriasis lichenoides acuta: high-power view showing fibrinoid necrosis affecting the dermal vasculature.