Erythema multiforme
Erythema multiforme
Clinical features Erythema multiforme is a relatively common condition, which predominantly affects younger individuals (particularly in their second to fourth decades), including children, and shows a slight male predilection.1–8 All races may be affected. It is self-limiting and commonly recurrent (recurrent erythema multiforme), although rarely continuous episodes of erythema multiforme have been described (persistent erythema multiforme).9–13 Very occasionally, epidemics are seen, for example, in military camps.4 The eruption shows seasonal variation with many patients developing the condition in spring and summer.
eventually blister. Although lesions are often present for up to 7 days, the entire episode is usually over by 6 weeks or less.14 Lesions often number a hundred or more. Resolution may be associated with postinflammatory hyperpigmentation.
It presents as symmetrically distributed, fixed, discrete erythematous round maculopapules 1–2 cm in diameter which appear in crops on the acral regions, particularly the elbows, the knees, and extensor aspects of the extremities (Figs 7.70–7.72). Sometimes, the face, palms and soles, flexural extremities, and perineum (Fig. 7.73) are affected.2 The scalp is rarely involved.14 Typically, the center of the lesions becomes ischemic to produce a bluish discoloration (the classic iris or target lesion), which may
Oral lesions are common and are usually mild, typically presenting as multiple ulcers, which may involve the entire oral cavity, or predominantly affect the buccal mucosa and tongue (Figs 7.74 and 7.75).15 Target lesions on the lips may also be encountered.
In many patients, episodes of erythema multiforme are recurrent, developing as often as five times each year. Such cases are almost invariably due to herpes simplex infection. Particular clinical features of this variant include a positive Koebner phenomenon, photodistribution, grouping of lesions over the elbows and knees, and nail fold involvement.8
In the older literature, a variant of erythema multiforme was recognized (erythema multiforme major) in which patients developed severe mucosal disease including oral, ocular, and anogenital lesions. In keeping with the current thinking on this complex topic, such cases are now included in the spectrum of Stevens-Johnson syndrome.1,2
Rarely, patients (usually females) may develop erythema multiforme in association with discoid or systemic lupus erythematosus – Rowell syndrome.
263 Interface dermatoses
including sulfonamides, trimethoprim- sulfamethoxazole combinations, penicillin, barbiturates, oral contraceptives, TNF-α antagonists, bortezomib, sorafenib, antiretroviral drugs in HIV patients, ciprofloxacin, and terbinafine.4,1,28–35 An interesting association with ciprofloxacin after alcohol ingestion has been described.34 The antineoplastic drug paclitaxel has not only been associated with erythema multiforme but may trigger a photosensitive variant of the disease.36 Furthermore, the eruption has also been associated with photocontact dermatitis to ketoprofen and statins and as a result of contact to hair dyes.37–41 A localized contact dermatitis to a henna tattoo has also triggered the disease.42 Erythema multiforme has also been associated with internal malignancy, including lymphoma, and may follow radiotherapy.43–46
Pathogenesis and histologic features
The etiology in the overwhelming majority of cases is past or present infection with herpes simplex virus (HSV) types I and II. In many patients, disease is subclinical. In some studies, the relationship is strongest in patients with recurrent disease. Mycoplasma infection is also of etiological importance. Many other infections have been implicated including orf, cowpox, Epstein–Barr virus, HIV, streptococcus, meningococcus, Histoplasma, Leishmania, and various vaccinations including those for meningitis, human papillomavirus, influenza, varicella, and hepatitis B.4,14,16–27 Some of these might be better classified as some other dermatosis, including Stevens-Johnson syndrome. Erythema multiforme has also been described as a side effect of a number of drugs, an incomplete list
Although cultures of skin lesions in erythema multiforme are generally negative for herpes simplex, viral DNA has been identified within the epidermis of skin lesions by polymerase chain reaction (PCR); in situ hybridization and immunohistochemistry detecting viral components are often positive.13,16,47–54 Viral DNA is absent from healed lesions.50 Viral gene expression correlates with lesion development.48 As there is no evidence of a viremia, it is thought that viral DNA is transported to the skin within circulating lymphocytes rather than directly through the bloodstream or via centrifugal neuronal spread.50,53 Why it localizes to specific sites in the skin
264 Lichenoid and interface dermatitis
is unknown but this may be related to ultraviolet (UV) exposure. It is likely that an episode of erythema multiforme develops as a delayed hypersensitivity (and/or cytotoxic) reaction to herpes viral antigens including DNA polymerase expressed on the surface of keratinocytes. The identification of IFN-γ in active skin lesions suggests a delayed hypersensitivity reaction with involvement of variable cytokines recruiting additional lymphocytes and macrophages to amplify the inflammatory reaction.54,55 It has been postulated that HSV DNA polymerase might also be associated with increased expression of transforming growth factor-beta (TGF-β) and p21waf, thereby accounting for cell growth arrest and apoptosis.56 Viral antigens do not persist in lesional skin after resolution of the eruption, and therefore in patients with recurrent disease, repeat transportation of viral DNA to the skin must occur.
Erythema multiforme is associated with an increased incidence of HLA-B15 (B62), HLA-B35, and HLA-DR53, particularly in recurrent disease.57–60 Patients with limited mucosal involvement show an increased frequency of HLA-DQB10302 compared with patients in whom mucosal lesions predominate, when HLA-DQB10402 is more commonly identified.60
Erythema multiforme is characterized by a combination of basal cell hydropic degeneration and keratinocyte apoptosis accompanied by a mild to moderate superficial dermal lymphohistiocytic infiltrate associated with lymphocytic exocytosis and satellite cell necrosis.16,61–65 Typically, the epidermis lacks parakeratosis or hyperkeratosis, and the presence of a normal stratum corneum can be a clue to the diagnosis. An exceptional case in which the predominant cells were histiocytes mimicking Kikuchi disease has been described.66
Apoptotic keratinocytes are rounded, intensely eosinophilic, and often anucleate, although residual pyknotic forms may be present (Figs 7.76 and 7.77). Their distribution may be focal, involving only an occasional and often basally located keratinocyte, or it can affect the entire epidermis, thereby resembling toxic epidermal necrolysis (Lyell syndrome) (Fig. 7.78). Marked basal cell hydropic degeneration sometimes results in subepidermal clefting or vesiculation (Fig. 7.79). Intra- and intercellular intraepidermal edema is evident and spongiotic vesiculation can be a feature (Fig. 7.80).
In biopsies from early lesions, the changes may be predominantly dermal with marked edema of the papillary dermis accompanied by a chronic inflammatory cell infiltrate and red cell extravasation (Fig. 7.81), thereby accounting for the clinical appearance of purpura. A vasculitis, however, is not seen.
The inflammatory cell infiltrate in erythema multiforme usually comprises lymphocytes and histiocytes; neutrophils are sparse or absent. Eosinophils may sometimes also be present.67,68 Leukocytoclasis is not a feature.
Histologic features, similar to those of the skin lesions, typify involvement of the mucous membranes with spongiosis and intracellular edema.
265 Interface dermatoses
subacute cutaneous lupus erythematosus and dermatomyositis. Presence of mucin and evidence of chronicity such as hyperkeratosis and parakeratosis are useful clues for connective tissue disease. The presence of numerous eosinophils would be in favor of a drug reaction. Focal interface change combined with an absence of significant eosinophils and follicular involvement is thought helpful for distinguishing between GVHD and erythema multiforme. None of the findings is considered absolutely pathognomonic of any entity, and clinicopathological correlation will most often ensure their distinction with ease.
These lesions tend to be more obvious and, therefore, intraepithelial blisters are sometimes conspicuous.
With immunohistochemistry, the infiltrate consists predominantly of helper (CD4+ Vβ2+) lymphocytes with a lesser number of cytotoxic lymphocytes and admixed macrophages.69,70 Keratinocytes express intracellular adhesion molecule-1 (ICAM-1) and HLA-DR; the latter is thought to be induced by IFN-γ of activated CD4+ T-helper 1 (Th1) cell derivation.69,71 TNF-α is not expressed in HSV-associated lesions.56 Circulating soluble Fas is thought to be a mediator of apoptosis, as in toxic epidermal necrolysis and Stevens-Johnson syndrome. Autantibodies to desmoplakin 1 and 2 may also play a role in erythema multiforme major.16

Fig. 7.70 Erythema multiforme: multiple lesions on the hand, a typical site of presentation. From the collection of the late N.P. Smith, MD, the Institute of Dermatology, London, UK.

Fig. 7.71 Erythema multiforme: multiple ulcerated lesions on the hands. From the collection of the late N.P. Smith, MD, the Institute of Dermatology, London, UK.

Fig. 7.72 Erythema multiforme: more extensive involvement in an adult with large erythematous lesions. The blisters have ruptured. By courtesy of the Institute of Dermatology, London.
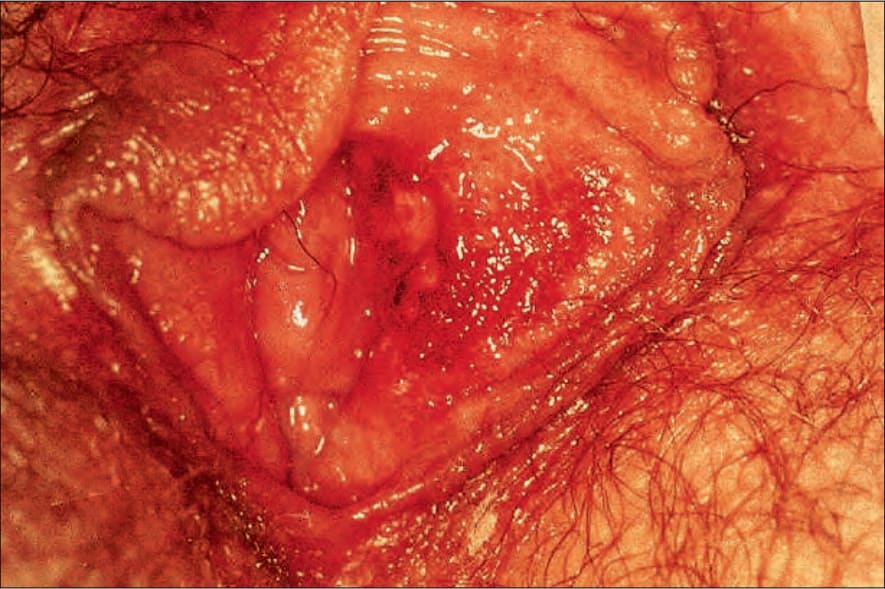
Fig. 7.73 Erythema multiforme: note the presence of erythema and erosion on the labium minus. By courtesy of P. Morgan, MD, London, UK.

Fig. 7.74 Erythema multiforme: multiple erosions are present on the labial mucosa. By courtesy of P. Morgan, MD, London, UK.
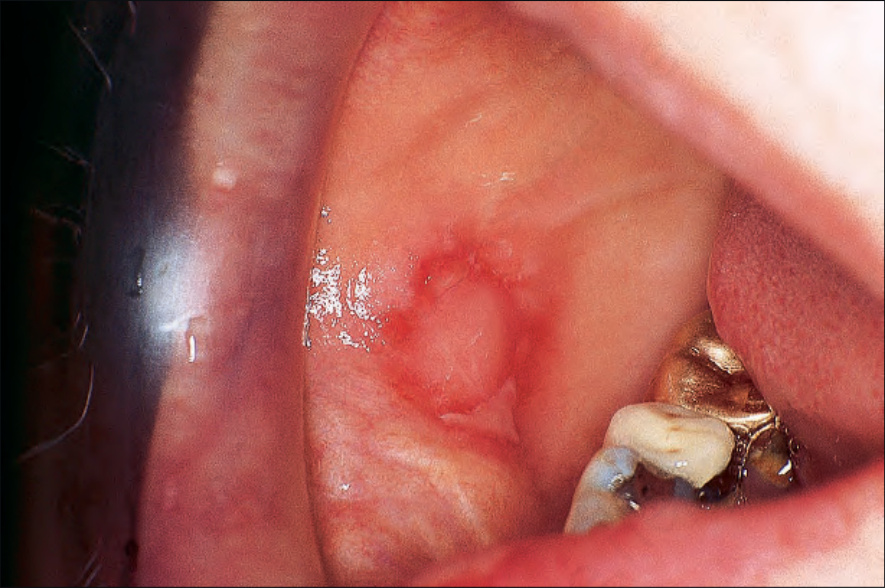
Fig. 7.75 Erythema multiforme: there is a large ulcer on the buccal mucosa. By courtesy of P. Morgan, MD, London, UK.
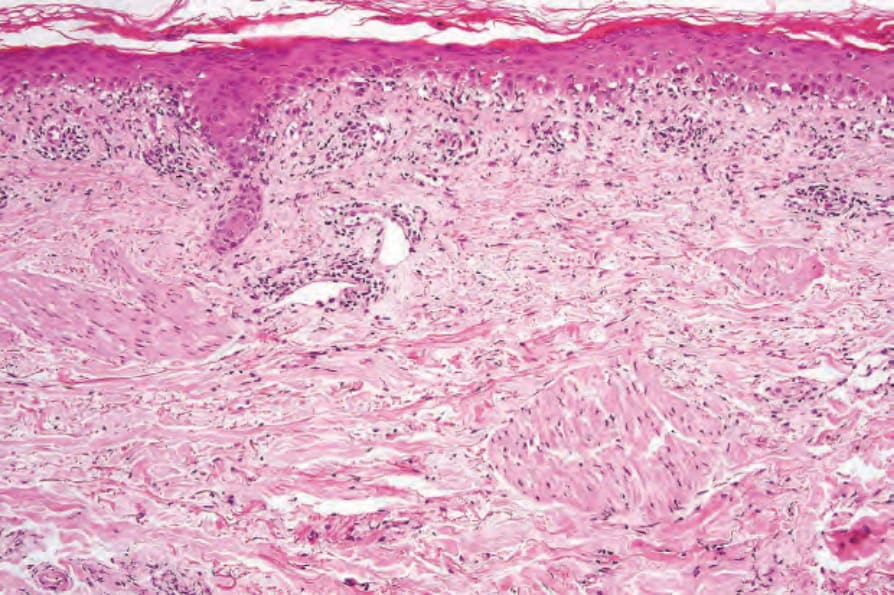
Fig. 7.76 Erythema multiforme: early lesion showing hyperkeratosis, basal cell hydropic degeneration, and occasional cytoid bodies.
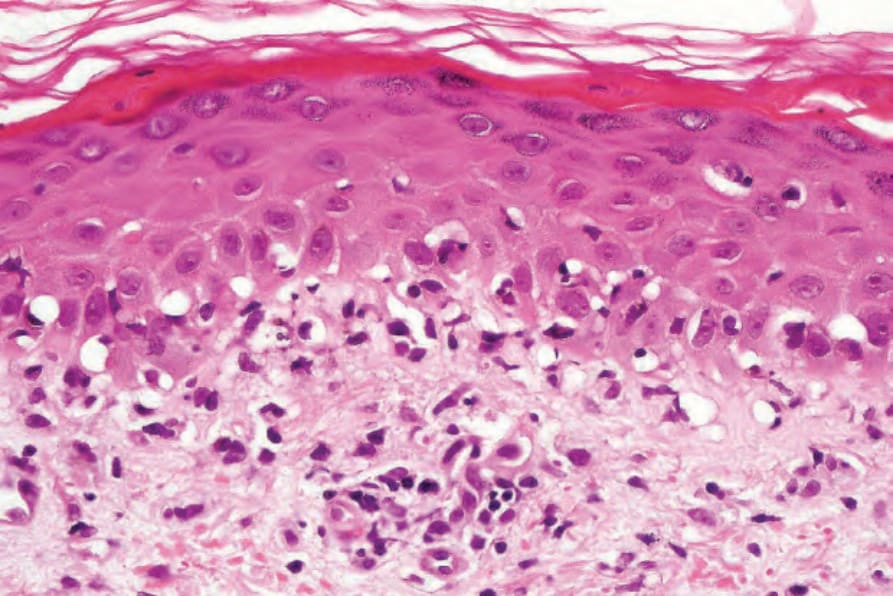
Fig. 7.77 Erythema multiforme: close-up view of basal cell hydropic degeneration.
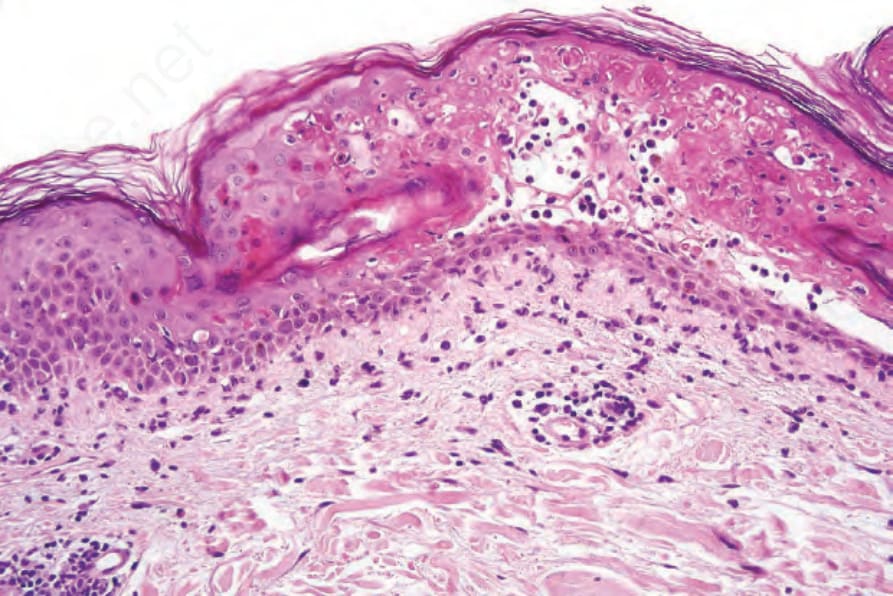
Fig. 7.78 Erythema multiforme: marked apoptosis has resulted in intraepidermal vesiculation.
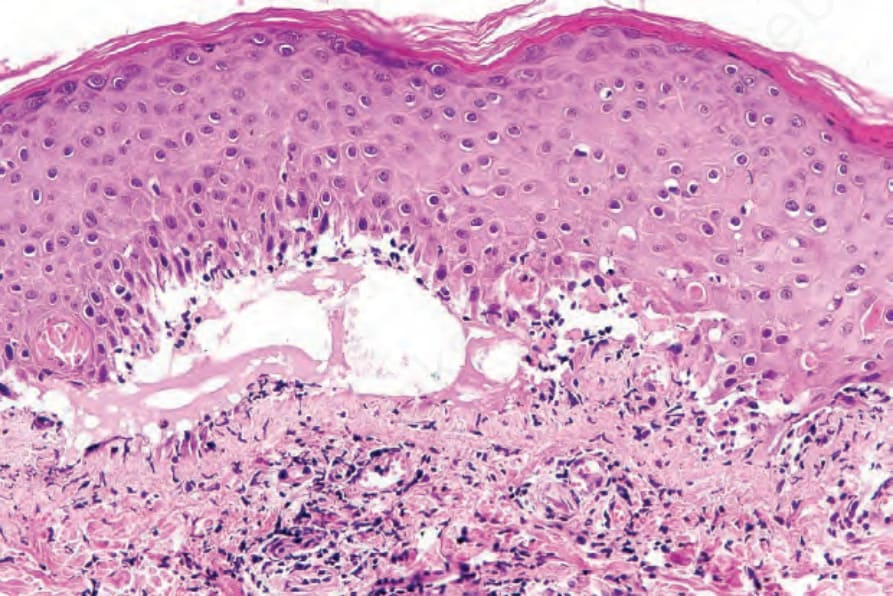
Fig. 7.79 Erythema multiforme: in this example, subepidermal vesiculation is present.
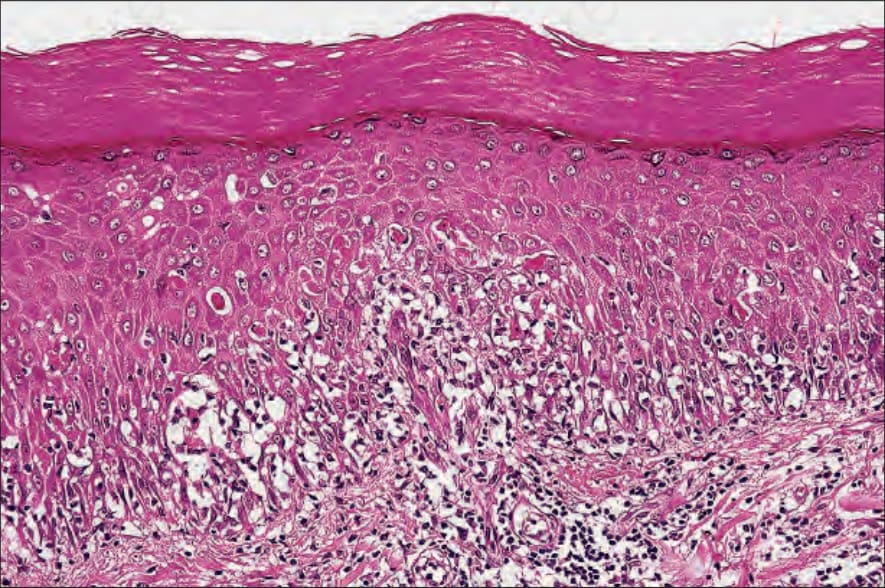
Fig. 7.80 Erythema multiforme: early lesion showing spongiosis, lymphocytic exocytosis, and cytoid bodies.
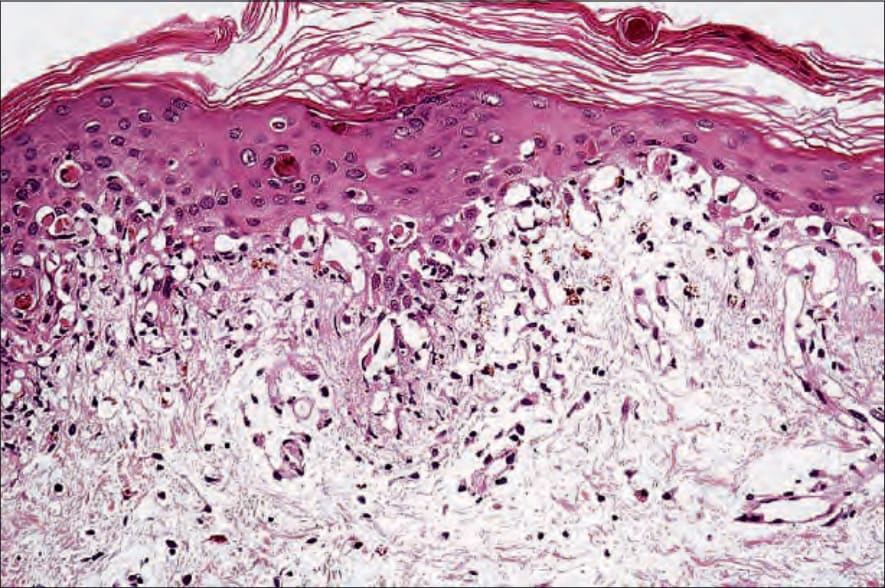
Fig. 7.81 Erythema multiforme: early lesion showing interface change and marked upper dermal edema.

Fig. 7.82 Stevens-Johnson syndrome: this patient developed Stevens-Johnson syndrome following sulfonamide therapy. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.