Annular lichenoid dermatitis (of youth)
Annular lichenoid dermatitis (of youth)
Clinical features Annular lichenoid dermatitis of youth is a chronic condition that most commonly presents in children, with a median age of 10 years, but cases in very young children and adults have been described.1–8 There appears to be no sex predilection, although adult cases appear to be more common in men.4 The recognition of cases in adults have prompted the suggestion that the terminology be changed to annular lichenoid dermatitis.4 The lesions vary from erythematous macules to the more common red-brown, annular, nonindurated patches with central hypopigmentation.1–8 The most common sites are the groin and trunk, especially the flanks, but lesions on the buttock, abdomen, and occasionally neck have been described. Most patients have multiple patches in the involved skin, but solitary lesions have also been documented. Most are asymptomatic with occasional patients reporting intermittent pruritus.2
Pathogenesis and histologic features The pathogenesis is unknown, but it does not appear to be related to parvovirus, Epstein-Barr virus, cytomegalovirus, or Borrelia infections, although one study has implicated Borrelia infection in Austrian patients based on serologic studies.1,4,9 Patch testing has not revealed a contactant trigger.1,10 A single case temporally associated with hepatitis B vaccination
has been reported, but this may be coincidental, as no other reported case has been associated with vaccination.11
Microscopically, the epidermis is not spongiotic and has a normal to slightly hyperkeratotic stratum corneum without parakeratosis and a normal granular layer. Within the epidermis, there is a bandlike lymphocytic infiltrate with basal vacuolization and frequently numerous necrotic keratinocytes exclusively at the tips of the rete (Fig. 7.64).1,4,7 The keratinocyte necrosis often results in a squared-off, quadrangular appearance of the rete (Fig. 7.67). Variable numbers of melanophages may be present.
In the initial description, immunohistochemical studies showed that the majority of the dermal lymphocytes are composed of CD4+ T cells, with few CD8+ lymphocytes.1 Subsequent studies have shown that the majority of the intraepidermal lymphocytes are CD8+ cytotoxic T cells.2,4,7,12 In some
261 Interface dermatoses
mycosis fungoides, the lymphocytes often are associated with perinuclear haloes that, with rare exceptions, are absent in annular lichenoid dermatitis of youth.12 The lymphocytes in mycosis fungoides often demonstrate irregular nuclei. Atypia of lymphocytes in annular lichenoid dermatitis of youth is absent to only focally present. Mycosis fungoides may have necrotic keratinocytes, but does not have them concentrated at the rete tips or the quadrangular rete tips. Importantly, the infiltrate in annular lichenoid dermatitis of the youth has been polyclonal in every case tested.1,2,4,7,12 Inflammatory morphea lacks interface change and still often shows some dermal fibrosis. Early lichen sclerosus has interface change, but not with prominent necrosis of keratinocytes at the rete tips. Early lichen sclerosus has a thickened basement membrane and does not have squared-off rete ridges. The inflammatory phase of vitiligo has a more diffuse pattern without the prominent epidermal damage concentrated at the tips of the rete.
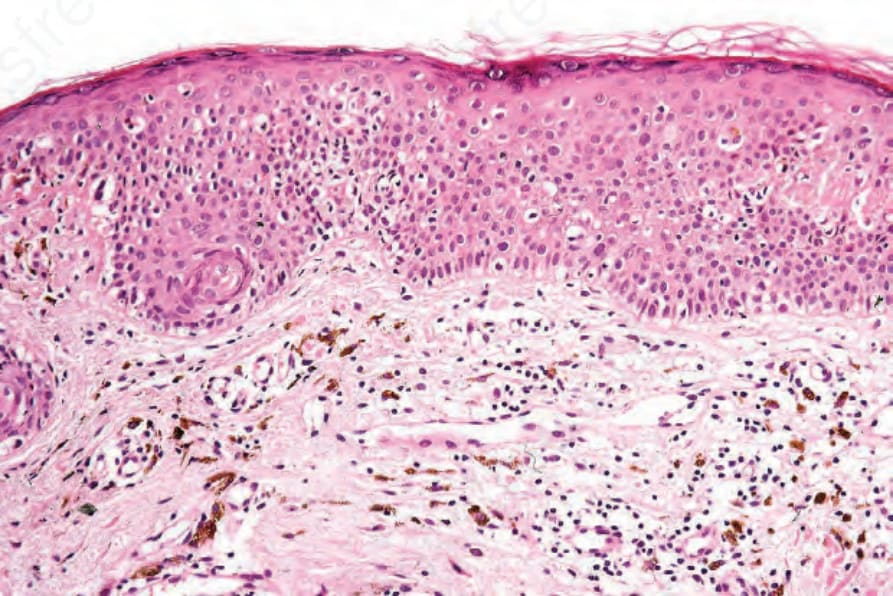
Fig. 7.64 Erythema dyschromicum perstans: there is hyperkeratosis and marked pigmentary incontinence.
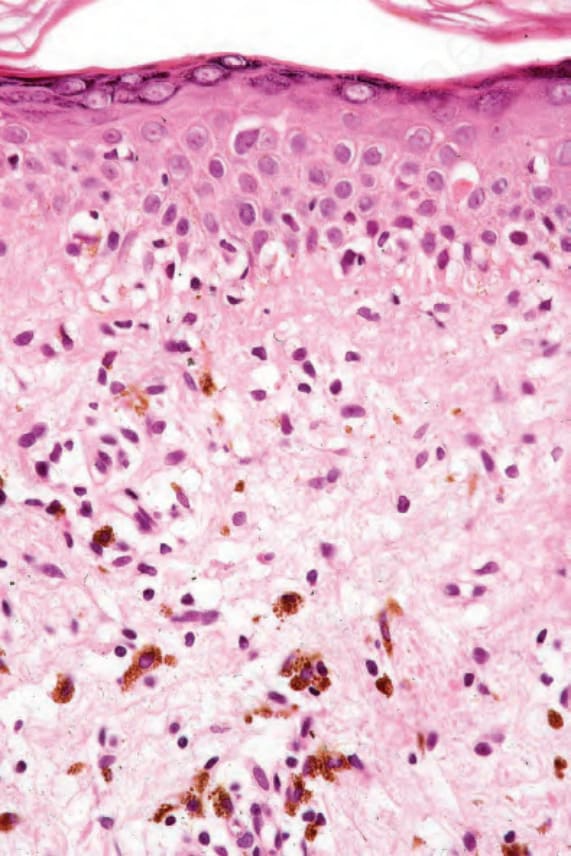
Fig. 7.65 Erythema dyschromicum perstans: note the hydropic degeneration, cytoid body, and pigment incontinence.
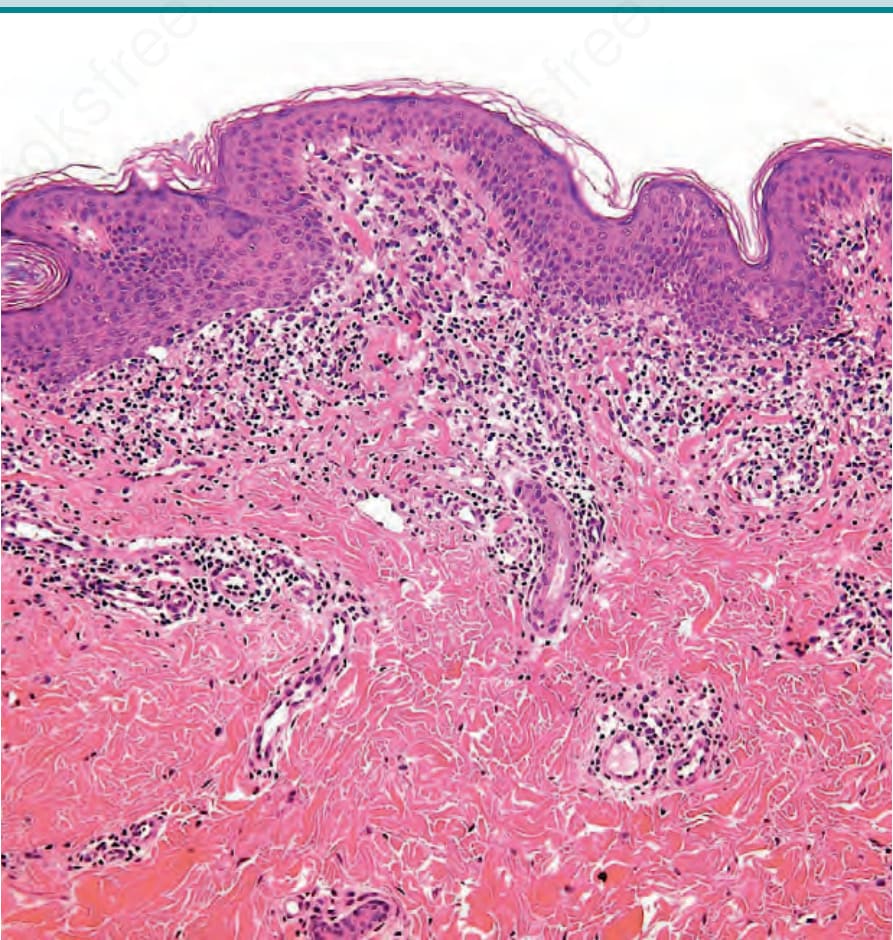
Fig. 7.66 Annular lichenoid dermatitis of youth: there is a lichenoid lymphocytic infiltrate that is concentrated at the tips of the rete. By courtesy of Dr. Carlo Tomasini, Torino, Italy.
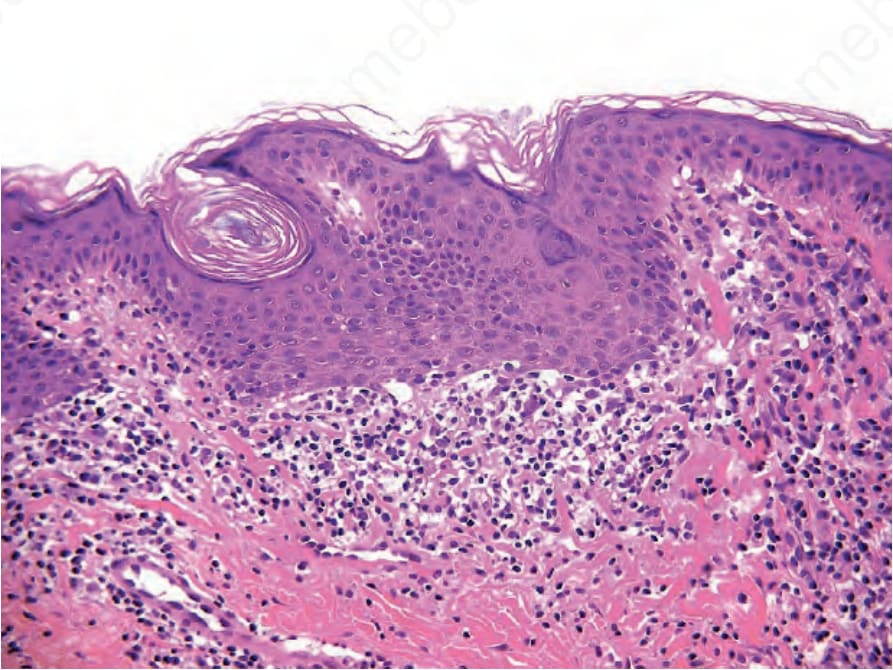
Fig. 7.67 Annular lichenoid dermatitis of youth: the infiltrate causes epidermal necrosis concentrated at the tips of the rete resulting in squared-off, quadrangular rete. By courtesy of Dr. Carlo Tomasini, Torino, Italy.
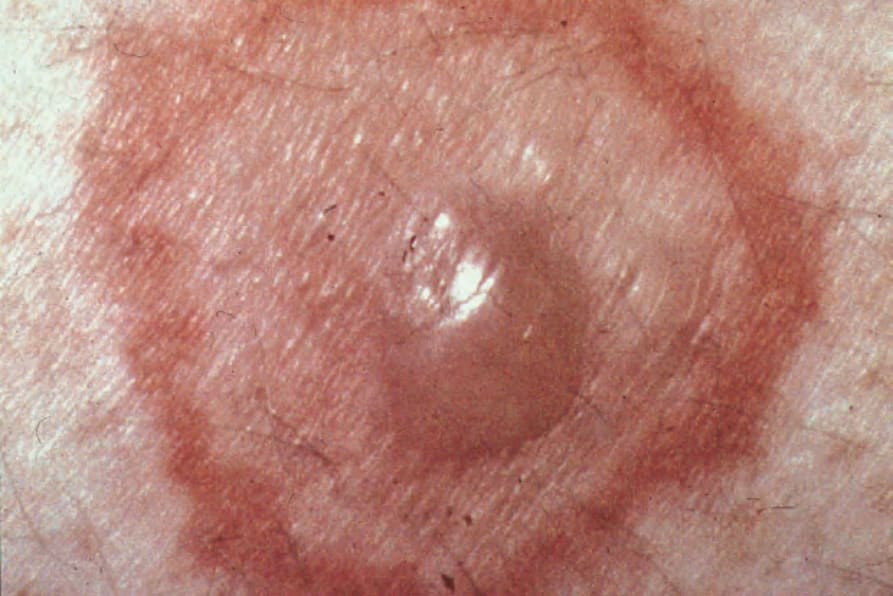
Fig. 7.68 Target lesion: characterized by a central blister surrounded by an edematous ring and an outer erythematous border. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.