Erythema dyschromicum perstans
Erythema dyschromicum perstans
Clinical features Erythema dyschromicum perstans (dermatosis cenicienta, ashy dermatosis) is an acquired, usually asymptomatic, disfiguring dermatosis which occurs particularly in Latin American (especially Mexican) populations and in Asians.1–8 It was originally named dermatosis cenicienta after the clinical appearance of affected patients – los cenicientos (the ash-colored ones).1 However, white-skinned races may rarely be affected.9–11 It is of unknown
Sections from the inflammatory border show hyperkeratosis and an epidermis of normal thickness or somewhat atrophic, accompanied by basal cell hydropic degeneration and cytoid body formation (Fig. 7.62). Pigmentary incontinence is marked, and a mild perivascular or lichenoid inflammatory cell infiltrate is present in the superficial dermis (Fig. 7.63). Sections from the central gray area show epidermal atrophy, follicular hyperkeratosis, and pigmentary incontinence. Often, biopsies are obtained from late lesions, with the only feature noted that of prominent pigment incontinence. The dermal inflammatory infiltrate is composed of both CD4 and CD8 T cells, usually with CD8 forms slightly predominating.17
Direct immunofluorescence reveals a pattern similar to lichen planus, with non-specific staining of the cytoid bodies with IgG, IgM, and C3, and
259 Lichenoid dermatoses
260 Lichenoid and interface dermatitis
fibrinogen deposition at the dermal–epidermal junction.18–20 The epidermal keratinocytes express Ia antigen, and the lymphocytic population comprises both helper/inducer and suppressor/cytotoxic phenotypes similar to lichen planus.20,21
Ultrastructural findings are non-specific, comprising intra- and interepidermal edema with cytoplasmic vacuolation, separation of keratinocytes, retraction of desmosomes, cytoid body formation, focal gaps in the keratinocyte basal lamina, and pigment-laden histiocytes in the papillary dermis.19,22,23
Differential diagnosis The precise relationship of erythema dyschromicum perstans to lichen planus is uncertain. The histologic, immunological, and ultrastructural findings certainly suggests a relationship.18,19 Typical lichen planus may precede the development of erythema dyschromicum perstans and sometimes the two conditions have presented simultaneously, although some of the documented cases may have represented lichen planus pigmentosus.24–26

Fig. 7.60 Keratosis lichenoides chronica: plantar involvement showing disfiguring exophytic, hyperkeratotic verrucous plaques. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.

Fig. 7.61 Erythema dyschromicum perstans: this patient shows irregularly distributed gray macules. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.
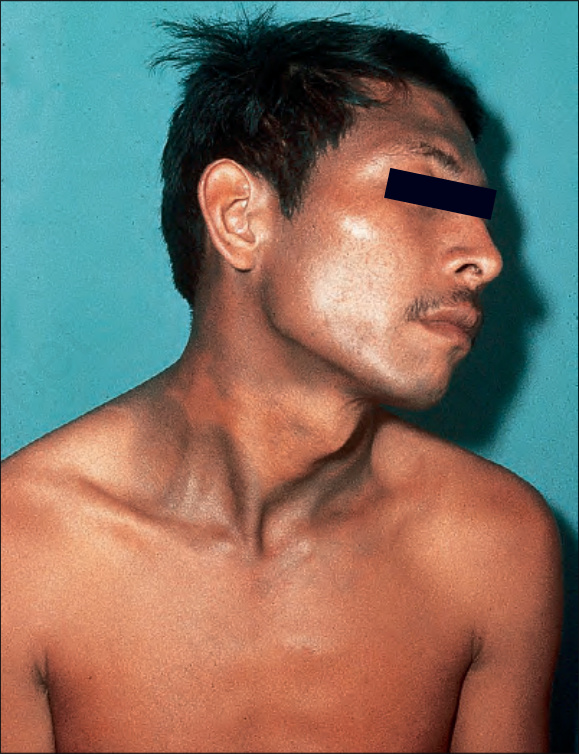
Fig. 7.62 Erythema dyschromicum perstans: in this patient, there is extensive involvement of the face, neck, and trunk. By courtesy of J. Tschen, MD, Baylor College of Medicine, Houston, USA.

Fig. 7.63 Erythema dyschromicum perstans: in this patient with more advanced disease, there is a generalized bluish discoloration. By courtesy of the Institute of Dermatology, London, UK.