Keratosis lichenoides chronica
Keratosis lichenoides chronica
Clinical features Keratosis lichenoides chronica (Nekam disease, lichen ruber verrucosus et reticularis) is a rare, chronic inflammatory dermatosis that combines the features of a seborrheic dermatitis-like eruption of the scalp and face with a progressive often reticular, lichenoid papulonodular dermatosis affecting the trunk, buttocks, and limbs.1–6 Patients usually present in the third to fifth decades although exceptionally reports of pediatric involvement have been documented, some with possible familial association.7–11 It may be persistent, but improvement can be seen in summer months and with phototherapy and/or systemic retinoids.5,12,13
Facial and scalp lesions are erythematous, greasy and scaly, and bear no resemblance to those found on the trunk and extremities, which are erythematous or violaceous lichenoid scaly papules in a confluent, reticulate, or linear distribution. The latter may suggest Koebner phenomenon (Fig 7.58). Papulonodular and infiltrated plaques are sometimes also present. Lesions are typically bilateral, symmetrical, and usually asymptomatic although rarely pruritus may be intense. Scarring is not a feature. Associated features include oral papules and ulceration, ocular lesions (blepharitis, conjunctivitis, anterior uveitis, and iridocyclitis), laryngeal nodules, palmoplantar keratoderma, and nail changes including yellow discoloration and dystrophy (longitudinal ridging, nail plate thickening, onycholysis, and paronychia) (Fig. 7.60).1,14–17 Genital involvement including penile and scrotal papules, chronic balanitis, and phimosis has been documented.6,15,16
Pathogenesis and histologic features The etiology is unknown. Abnormalities in chromosome 18 in cells from involved skin in comparison to normal-appearing skin has been described in a female patient with adult Blaschkitis, supporting a link with cutaneous genetic mosaicism.13 Association with drugs and emotional stress has been reported.11,12,15,16
Keratosis lichenoides chronica has been described in association with a number of systemic diseases including chronic infections (toxoplasmosis, tuberculosis, and viral hepatitis), kidney disease, and lymphoma.3,18–21
258 Lichenoid and interface dermatitis
Pathogenesis and histologic features
etiology, shows a female predilection, and can develop at any age, although the majority of patients are in their first three decades.2,8,12 Presentation in infancy has been documented.13
The precise nature of keratosis lichenoides chronica is uncertain. Although some authors regard it as a variant of hypertrophic lichen planus, this is unlikely.10,22
Histologically, the lichenoid eruption is characterized by hyperkeratosis and parakeratosis, variable acanthosis, and epidermal atrophy associated with a bandlike lymphohistiocytic infiltrate in the superficial dermis, often with conspicuous melanophages.15 Neutrophils may be prominent in the stratum corneum. Perifollicular/acrosyringotropic and perivascular chronic inflammation may also be evident. Epidermal basal keratinocytes show hydropic degeneration, and cytoid body formation has been described.15,22 Many necrotic keratinocytes are present.1 Exceptionally, amyloid deposition has been documented.23
The dermal infiltrate consists of lymphocytes, histiocytes, and variable plasma cells and eosinophils.15
Patients develop oval, irregular or polycyclic, gray macules with erythematous, indurated, inflammatory borders of 1–2 mm. The lesions extend peripherally, show a tendency to coalesce, and often affect large areas of the integument (Figs 7.59–7.61). With progression, the eruption develops a gray-blue color and loses the erythematous border, which is sometimes replaced by a hypopigmented periphery. It is usually symmetrical, and particularly affects the trunk, proximal extremities, and, to a lesser extent, the face and neck.2,8 The palms and soles, scalp, nails, and mucous membranes do not appear to be involved.6
Pathogenesis and histologic features The etiology is unknown. Cases have followed HIV infection, and there is a report of simultaneous development of vitiligo and erythema dyschromicum perstans. The significance of these observations is doubtful.14,15 Increased susceptibility with HLA-DRB1*0407 in Mexican patients has been reported.16
Direct immunofluorescence highlights the cytoid bodies.22
The scalp and facial lesions show the features of a chronic dermatitis, namely, spongiosis with exocytosis and patchy parakeratosis. A perivascular chronic inflammatory cell infiltrate of lymphocytes, histiocytes, and plasma cells may be present in the upper dermis.5
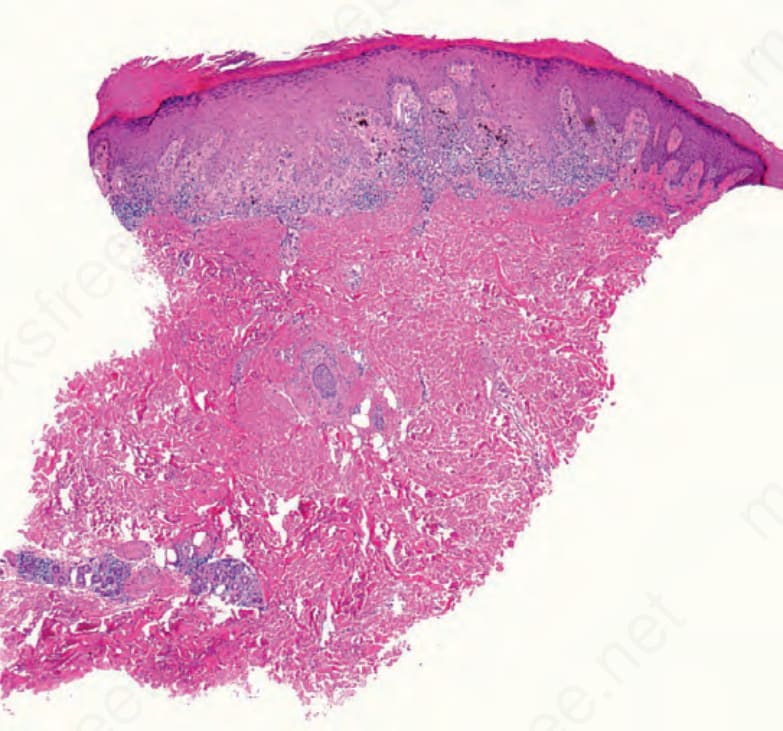
Fig. 7.56 Lichen striatus: the scanning image demonstrates a lichenoid interface dermatitis and a deeper perieccrine infiltrate.

Fig. 7.58 Keratosis lichenoides chronica: there are erythematous hyperkeratotic lichenoid lesions in a linear and reticular distribution. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.

Fig. 7.59 Keratosis lichenoides chronica: close-up view of solitary lichenoid papules and a confluent plaque. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.

Fig. 7.60 Keratosis lichenoides chronica: plantar involvement showing disfiguring exophytic, hyperkeratotic verrucous plaques. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.