Lichen striatus
Lichen striatus
Clinical features Lichen striatus [Blaschko linear acquired inflammatory skin eruption (BLAISE)] is an uncommon, usually asymptomatic, dermatosis of unknown etiology, affecting the limbs or neck in which lesions typically follow Blaschko lines.1–9 Infrequently, the condition is pruritic.6–8,11 It is self-limiting, normally disappearing within months to a year of onset. It shows a female predominance (2–3 : 1) and, although it may occur at any age, it most often presents in children aged 5–15 years.2,5,7,8 Rarely, lichen striatus has been described in adults (adult Blaschkitis, see below).4,10,12,13 Occurrence during pregnancy is very rare.14 A family history is rarely encountered, suggesting a genetic predisposition and/or a common environmental etiology in such cases.2,6,8,15,16 It is associated with seasonal variation with most series reporting the majority of patients presenting in spring and summer,2,7 with the exception of one large series where the majority of patients presented in the winter 8,15 Case clustering has been documented.2
autoimmune reaction to an abnormal clone of cells. Blaschko lines are believed to represent the direction along which epidermal growth centers expand during early skin development.1 It has been suggested that the distribution of lesions in lichen striatus may reflect a postzygotic abnormality such as somatic mutation affecting localized stem cells.1 An intriguing case following trauma in an adult has been reported.26 Further exceptional cases associated with solarium use, varicella and influenza infection, hepatitis B and BCG vaccine, interferon and etancercept therapy, and bee stings have been described.27–34
Lesions, usually solitary and unilateral, present as erythematous or flesh-colored lichenoid or sometimes psoriasiform scaly papules, which coalesce into a continuous or interrupted linear or curved band, 1–3 cm wide and often covering the whole length of a limb, either lower or upper extremities (Figs 7.50 and 7.51).2,8 Occasionally, multiple lesions have been recorded, as has bilaterality.8,17,18 Presentation at two different sites and at multiple sites may exceptionally occur.19 Nail changes, which may affect a single nail, include onycholysis, longitudinal ridging, splitting, and nail loss.1,8,20–22 Exceptionally, lichen striatus with bilateral nail dystrophy has been described.23,24 Lichen striatus is not associated with Koebner phenomenon. Hypo- or hyperpigmentation sometimes follows resolution, which may be marked in people with pigmented skin.8 Lichen striatus is associated with atopy in up to 60% of patients.1,6–8
The histologic features of lichen striatus may be non-specific and show changes of mild chronic non-specific dermatitis.35 In an established lesion, however, the changes often consist of an admixture of spongiotic dermatitis with lichenoid and interface features (Fig. 7.52).36 Thus, there is often parakeratosis with a normal or slightly acanthotic epidermis accompanied by intercellular edema, lymphocytic exocytosis, and keratinocyte necrosis (Figs 7.53–7.55). Satellite cell necrosis may sometimes be a feature, and transepidermal elimination of keratinocyte debris (perforating lichen striatus) has occasionally been documented.4,37 Intraepidermal Langerhans cell vesicles have exceptionally been described.36 A heavy lymphohistiocytic infiltrate is present in the superficial dermis and also surrounds the vessels of the superficial and deep vascular plexuses and sometimes also the cutaneous adnexae (Figs 7.56 and 7.57).4,36 Eosinophils and plasma cells are uncommon.36
Pathogenesis and histologic features The etiology of this condition is unknown although case clustering and seasonality raises the possibility of an environmental or infective basis in conjunction with an abnormal host response.2,25 The development of lesions along Blaschko lines also raises the possibility of a cell-mediated
Some biopsies may be indistinguishable from lichen planus. In those cases where there is follicular involvement, the features can resemble those of lichen planopilaris, and old lesions sometimes simulate lichen nitidus.
By immunohistochemistry, the majority of the intraepidermal lymphocytes are of a CD8+ cytotoxic phenotype.4,36 The dermal lymphocytes consist of an admixture of CD4+ and CD8+ subtypes. CD7 is typically conserved.29 Intraepidermal Langerhans cells may be normal, increased, or decreased.36
Nail changes include slight spongiosis with exocytosis, focal hypergranulosis, dyskeratosis, and a bandlike lymphohistiocytic infiltrate affecting the proximal nail fold, nail bed, and nail matrix dermis.20
256 Lichenoid and interface dermatitis

Fig. 7.50 Lichen striatus: a linear band of scaly hyperpigmented papules is present on the inner aspect of the leg, a commonly affected site. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.

Fig. 7.51 Lichen striatus: the arms are sometimes affected. The condition most often presents in children. By courtesy of the Institute of Dermatology, London, UK.
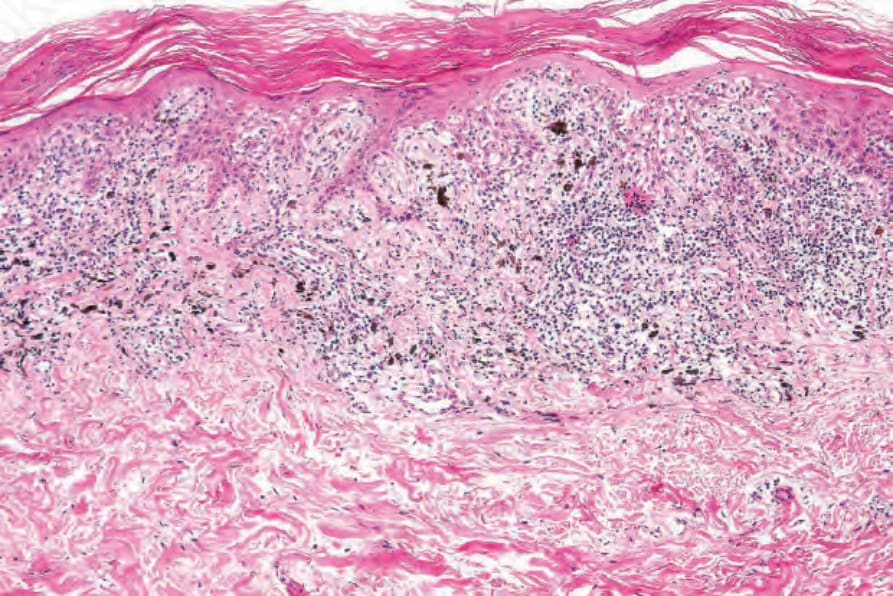
Fig. 7.52 Lichen striatus: scanning view showing hyperkeratosis, focal parakeratosis, and irregular acanthosis. A heavy inflammatory cell infiltrate is present in the upper dermis. There is conspicuous pigmentary incontinence. Case courtesy of S. Lyle, MD, Beth Israel Deaconess Medical Center, Boston, USA.
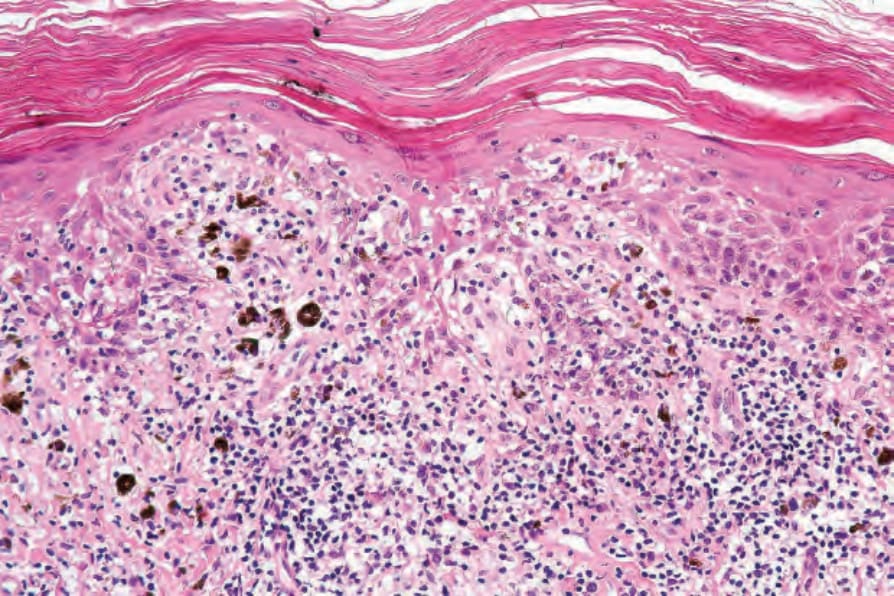
Fig. 7.53 Lichen striatus: in this field, there is parakeratosis, hyperkeratosis, spongiosis, and interface change. Note the pigment incontinence and intense chronic inflammatory cell infiltrate. Case courtesy of S. Lyle, MD, Beth Israel Deaconess Medical Center, Boston, USA.
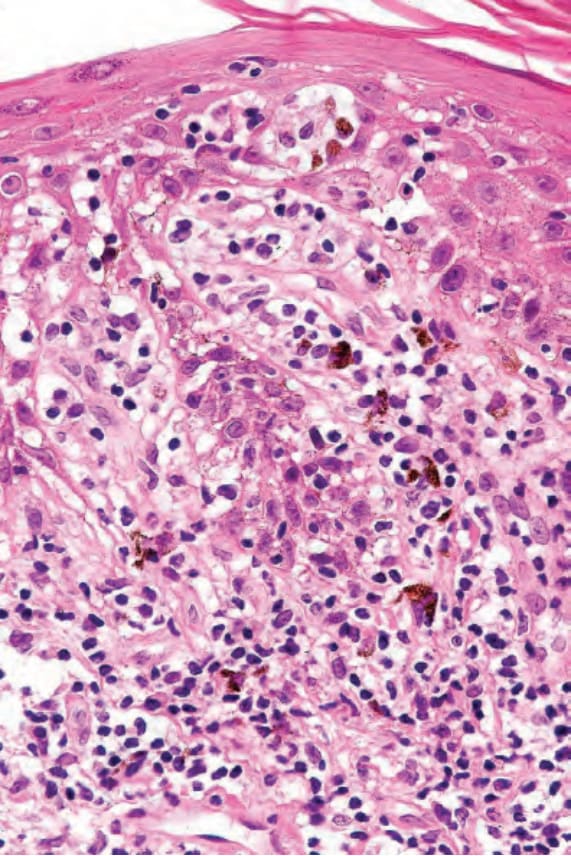
Fig. 7.54 Lichen striatus: there is spongiosis and marked lymphocytic exocytosis. Case courtesy of S. Lyle, MD, Beth Israel Deaconess Medical Center, Boston, USA.
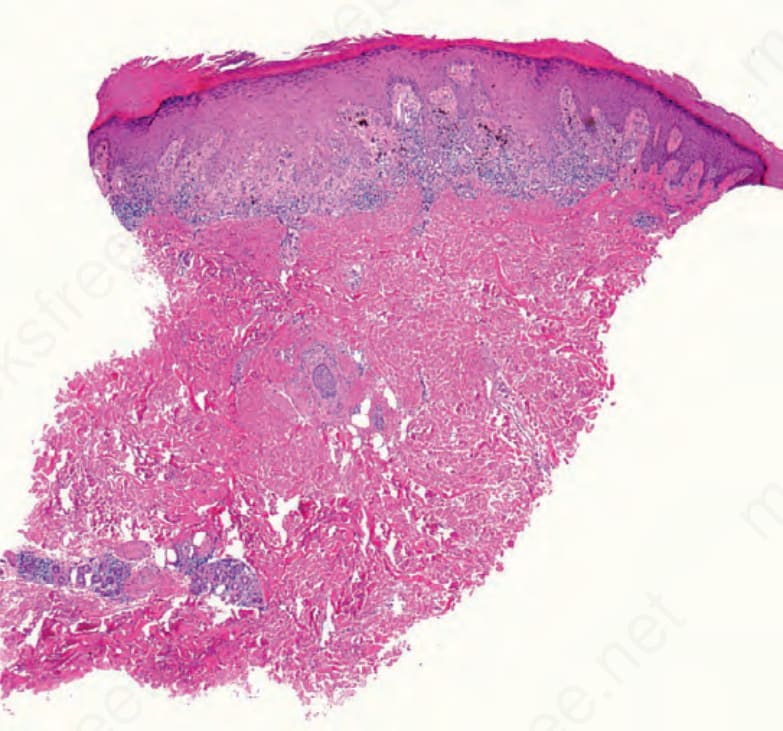
Fig. 7.56 Lichen striatus: the scanning image demonstrates a lichenoid interface dermatitis and a deeper perieccrine infiltrate.