Lichenoid keratosis
Lichenoid keratosis
Clinical features Lichenoid keratosis (benign lichenoid keratosis, lichen planus-like keratosis, solitary lichen planus) is not uncommon and usually presents as a solitary, 0.3–2-cm diameter, sharply demarcated, erythematous, violaceous, tan or brown papule or plaque (Fig. 7.44).1,2 Occasionally, multiple lesions may
Histologically, as its name suggests, the features are often very similar or even identical to those of lichen planus. There is hyperkeratosis, wedge-shaped hypergranulosis, variable acanthosis, and basal cell liquefactive degeneration sometimes accompanied by lymphocytic exocytosis (Figs 7.45 and 7.46).2,3,6,10 Foci of parakeratosis are also frequently seen.1,2,10 Although the sawtooth acanthosis of lichen planus is sometimes evident, more often the epithelium merely shows broadened, widened, and irregular epidermal ridges.5 The basal epidermal layers may sometimes show very minor degrees of cytological atypia, including cellular and nuclear enlargement with conspicuous nucleoli, but these changes represent regenerative phenomena.3 Dysplasia as seen in lichenoid actinic keratosis is not a feature of a lichenoid keratosis. Colloid bodies are usually conspicuous in both the epidermis and dermis, and pigmentary incontinence is often marked (Figs 7.47–7.49).1,2,8,10 Apoptotic keratinocytes can be prominent and may be associated with inatraepidermal blister formation with subepidermal
254 Lichenoid and interface dermatitis
vesiculation. In such cases, the histology can mimic conditions such as subacute cutaneous lupus erythematosus and even erythema multiforme. Epidermal pallor and dermal edema can be seen in cases with only slight or no acanthosis and an interface population of lymphocytes along the junction with vacuolar degeneration. Foci of atrophy can be occasionally encountered.2,10 In some cases, a combination of lichenoid and spongiotic changes may be seen.
A dense chronic inflammatory cell infiltrate is typically present in the superficial dermis. Although this characteristically has a lichenoid distribution, on some occasions it may be more discrete and predominantly perivascular in location.4,8 The infiltrate consists largely of lymphocytes and histiocytes, but small numbers of plasma cells and eosinophils are occasionally present. Exceptionally, atypical large T lymphocytes (enlarged with hyperchromatic, irregular, contoured nuclei) which are activated CD30 positive cells can be also seen.2 The adjacent dermis sometimes shows lentigo and solar elastosis. Features suggestive of mycoses fungoides such as Pautrier abscesses, dermal–epidermal tagging, and mild lymphocytic atypia have been exceptionally noted in benign lichenoid keratosis (lymphomatoid lichenoid keratosis).14 Clinicopathological correlation and careful follow-up are essential in such cases to avoid misdiagnosis.
Immunofluorescence findings, which are similar to those of lichen planus, comprise deposits of IgM and, less commonly, IgG outlining cytoid bodies.6
Differential diagnosis Many conditions show lichenoid histology and therefore come into the differential diagnosis. Most prominently, these include lichen planus and lichenoid drug reactions.
If clinical information is available, differentiation from lichen planus should present little difficulty. Lichen planus is characterized by large numbers of lesions in contradistinction to the single papule or plaque of lichenoid keratosis. In addition, lichen planus is usually itchy. Parakeratosis and dermal plasma cells are not usually a feature of lichen planus, but are more common of lichenoid keratosis.8
255 Lichenoid dermatoses
Both actinic keratoses and squamous cell carcinoma in situ may sometimes show a lichenoid inflammatory cell reaction. Dysplasia by definition is not a feature of lichenoid keratosis.1,2,10 Inflamed seborrheic keratosis and porokeratosis can have a prominent lichenoid reaction. The absence of horn cyst formation, squamous eddies, and laminated stratum corneum keratin helps distinguish these lesions from seborrheic keratosis, whereas the absence of cornoid lamella excludes porokeratosis. Melanocytic lesions with halo phenomenon can become a diagnostic consideration and require examination of the dermis and dermal–epidermal junction for melanocytic nests. In difficult cases, additional step sections or immunohistochemical studies can prove useful. Finally, the presence of scattered CD30-positive lymphocytes in some cases of lichenoid keratosis may raise the histologic differential diagnosis of lymphomatoid papulosis. However, the paucity of these enlarged CD30-positive cells, the absence of a deep infiltrate, and the clinically history of a solitary lesion is reassuring for lichenoid keratosis.2
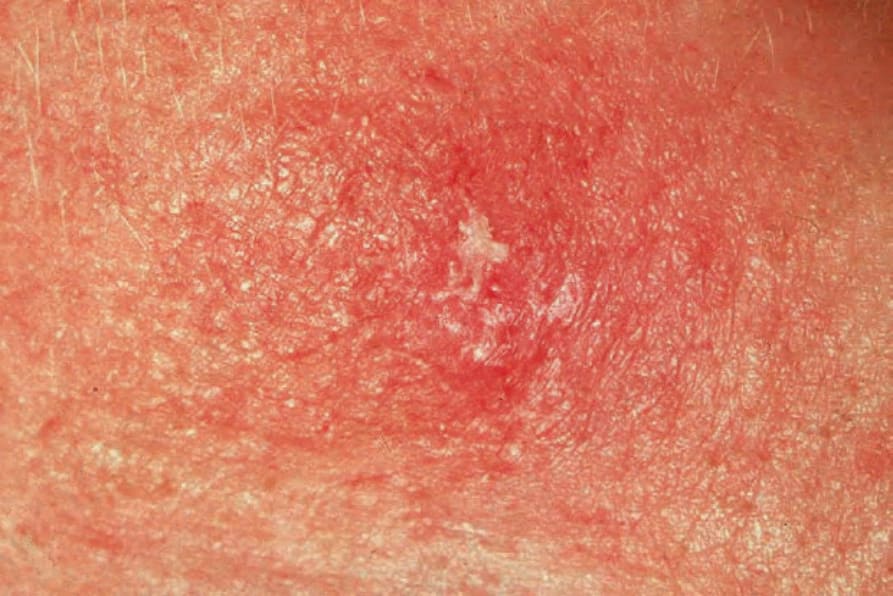
Fig. 7.44 Lichenoid keratosis: there is scaling overlying a slightly raised erythematous plaque. By courtesy of the Institute of Dermatology, London.
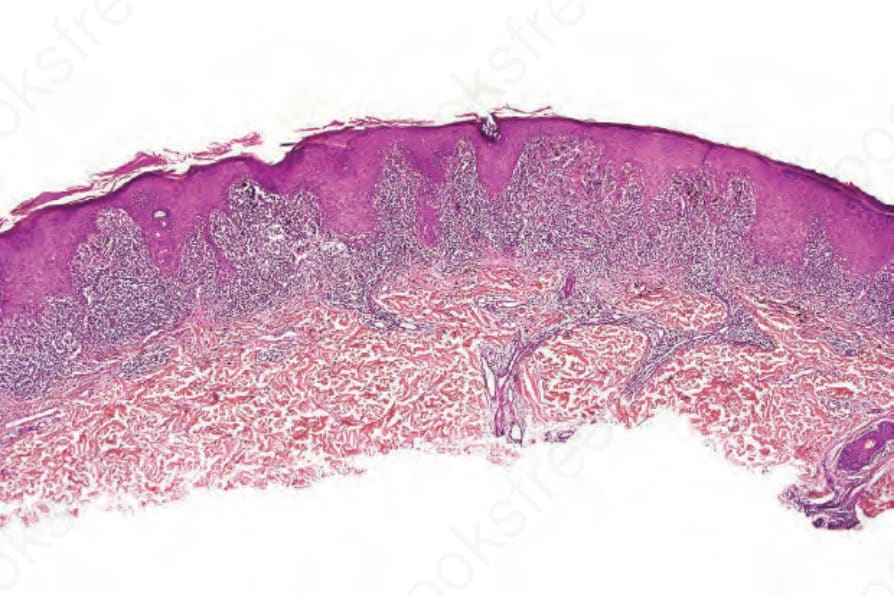
Fig. 7.45 Lichenoid keratosis: scanning view showing hyperkeratosis, hypergranulosis, irregular acanthosis, and a bandlike chronic inflammatory infiltrate.
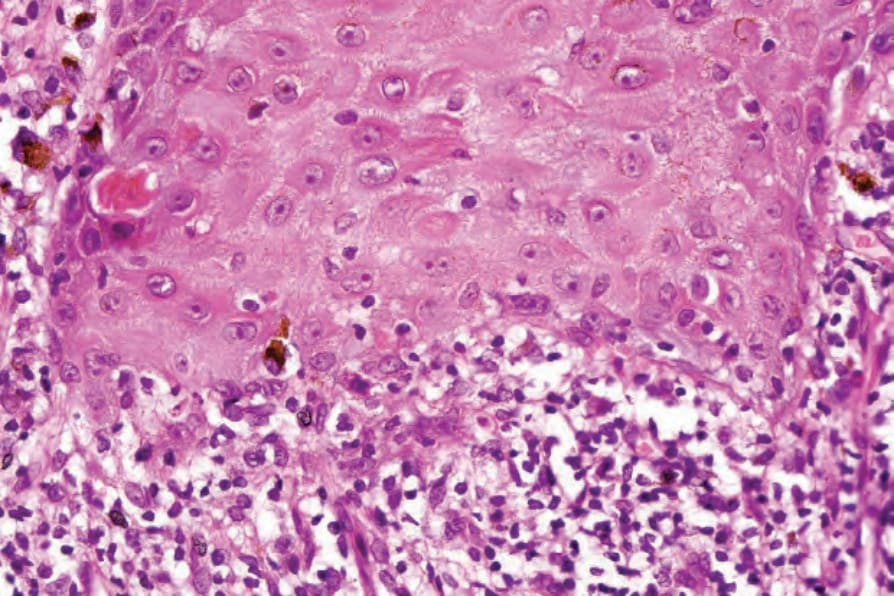
Fig. 7.46 Lichenoid keratosis: in this field there is basal cell liquefactive degeneration. Cytoid bodies are present.
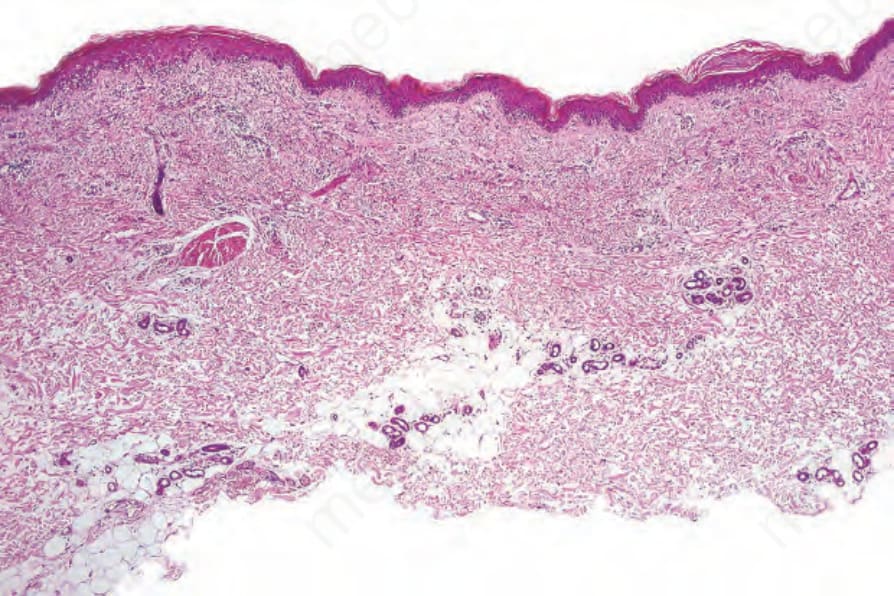
Fig. 7.47 Lichenoid keratosis: in this early lesion, there is more uniform acanthosis.
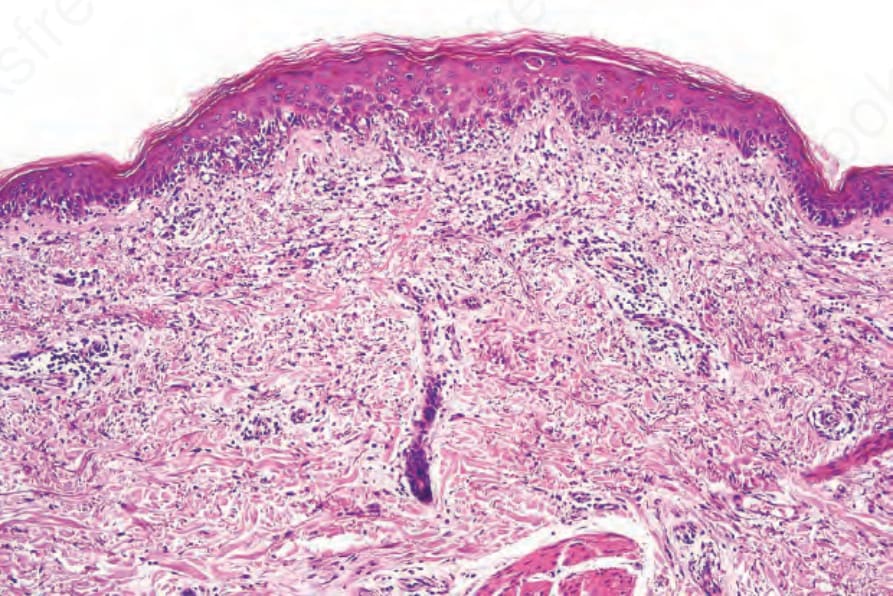
Fig. 7.48 Lichenoid keratosis: there is interface change with cytoid bodies.
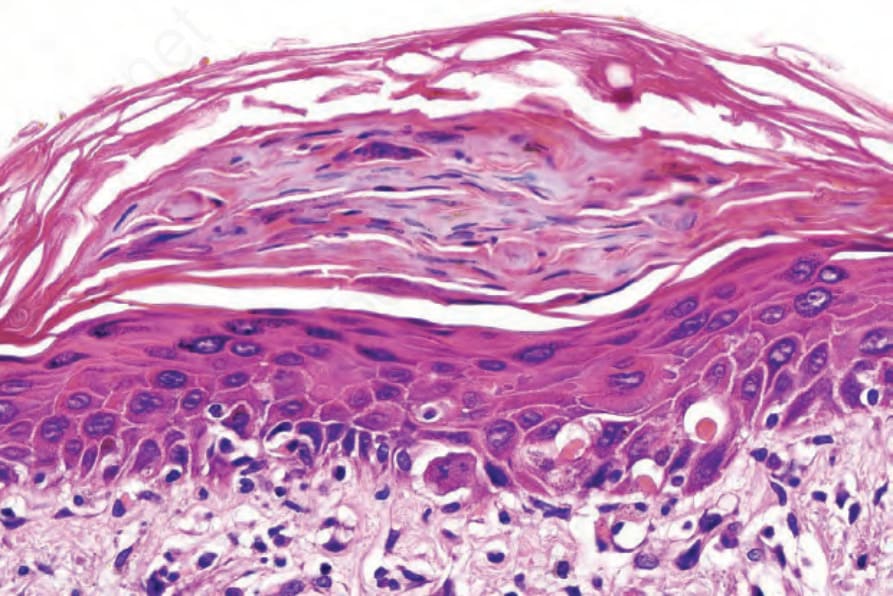
Fig. 7.49 Lichenoid keratosis: basal cell liquefactive degeneration is evident in addition to cytoid bodies. Note the parakeratosis.