Lichen nitidus
Lichen nitidus
Clinical features Lichen nitidus is a rare but distinctive dermatosis, which shows an equal sex incidence.1 Children and young adults are predominantly affected. It presents clinically as an eruption of pinhead-sized, flesh-colored, shiny, flat-topped or dome-shaped papules and shows a predilection for the arms, chest, abdomen, and genitalia (Figs 7.38 and 7.39).1–5 A positive Koebner
252 Lichenoid and interface dermatitis
phenomenon is typically present.5 The condition is usually localized and asymptomatic, although occasionally there may be mild or even intense pruritus.2 Rarely, generalized lesions have been described.2,6–9 An association with generalized lesions and Down syndrome has been documented, as has been a case after interferon-alpha therapy.8,9 Occasionally, papules may be encountered on the palms and soles.3–12 Familial cases have been rarely described.13,14 Lichen nitidus can spontaneously resolve within a few months or persist indefinitely.2
Mucosal involvement presenting as grayish-yellow papules has also been described.4 Nail involvement, which is rare, presents as thickening with ridges, rippling, terminal splitting, striations, and pits.2,4
Keratodermic, vesicular, hemorrhagic, purpuric, and perforating variants may rarely be encountered.2,15–19 Perforating lichen nitidus shows a predilection for the forearms and fingers, and may be trauma related.17,20,21
Actinic lichen nitidus refers to the development of lichen nitidus on sun-exposed sites, usually during the summer months. In some cases, involvement is predominantly facial and it may present in black patients.22 It shows considerable overlap with actinic lichen planus (see above).23,24
Histologic features Lichen nitidus is recognizable by a characteristic histology in many cases. The classic papule is sharply circumscribed and occupies the space of only four or five dermal papillae. It is often depressed in the center and composed of atrophic epidermis, frequently covered by a parakeratotic tier and overlying a cellular infiltrate (Figs 7.40–7.43). Clawlike extensions of epidermal ridges mark the lateral boundaries of the lesion. The epithelium shows basal cell hydropic degeneration, and cytoid bodies may be a feature. The inflammatory component consists of lymphocytes, histiocytes, and variable numbers of epithelioid cells. Giant cells are sometimes a feature and true granulomata may occasionally be found, although caseation is never present.25 A plasma cell-rich variant is exceptional. In addition to red blood cell extravasation, purpuric variants may show increased vascularity with vessel wall thickening and hyalinization.18 In rare cases, a prominent lymphocytic inflammatory infiltrate can extend down the hair follicle and eccrine glands, making the distinction from lichen striatus challenging.25 A
253 Lichenoid dermatoses
follicular variant of lichen nitidus may be seen and mimics lichen spinulosus histologically.26 However, rarely, lichen nitidus and lichen spinulosus may coexist clinically.27,28
Palmar lesions may be identical to those seen elsewhere or show a more diffuse bandlike upper dermal lymphohistiocytic infiltrate with associated giant cells and focal parakeratosis.3,10–12,29,30
Fibrin can be detected at the basement membrane zone by immunofluorescent techniques, but immunoglobulin deposition is not a feature.31,32 Immunophenotypic studies show that there is a marked excess of CD4+ cells (helper/inducer T cells) over CD8+ cells (cytotoxic/suppressor T cells).31 Langerhans cells are conspicuous.33 These findings are similar to those described for lichen planus.
be present.2–4 It is usually of short duration and shows a predilection for the face (particularly the cheeks and nose), neck, upper trunk (especially the presternal area), forearm, and dorsum of the hand.2,5–10 The surface is often scaly. Lesions are commonly asymptomatic, but mild pruritus has sometimes been documented.9 Patients are frequently Caucasian, but occasionally blacks are affected.2,8,9 Females develop these lesions more commonly than males, usually in their fourth to seventh decades.2,6,10
Lichenoid keratosis is often clinically misdiagnosed as a seborrheic keratosis, superficial basal cell carcinoma, squamous cell carcinoma, actinic keratosis, or Bowen disease.5
Pathogenesis and histologic features The precise nature of lichenoid keratosis is uncertain. In the past, it was regarded as a solitary lesion of lichen planus or thought to have an actinic pathogenesis.11–13 It was also proposed to represent an immunological or regressive response to a preexistent epidermal lesion similar to the phenomenon encountered with a ‘halo’ nevus.2 The frequent association of solar lentigines or, less commonly, seborrheic keratoses in the adjacent epithelium has been cited as evidence in favor of this hypothesis.5–7,9 Recent studies have shown the lymphocytic infiltrate in lichenoid keratosis to be immunophenotypically distinct from lichen planus. The lymphocytes in lichenoid keratosis are predominantly CD8-reactive in contrast to lichen planus. More CD20-positive B cells are usually seen in lichenoid keratosis. Furthermore, the lymphocyte infiltrate in lichenoid keratosis lacks the cutaneous lymphocyte antigen (CLA) expression, suggesting the absence of localized antigenic stimulation as seen in lichen planus.2,14 These studies suggest that lichenoid keratosis is distinct from lichen planus despite the similarities in histology.
Ultrastructural examination reveals rather non-specific findings including epidermal intercellular edema, subepidermal edema, colloid bodies, decreased numbers of desmosomes, and disruption or reduplication of the lamina densa.34–36 Perivascular electron-dense deposits (the nature of which is unknown) have been described in purpuric variants.8
Comment Lichen nitidus may coexist with lichen planus or predate it and lichen nitidus-like lesions may be found in patients with typical lichen planus, but it is unlikely that the conditions are closely related.37,38 Wickham striae are not a feature of lichen nitidus, and mucosal involvement is exceptional.2,4 Lichen nitidus is associated with parakeratosis and epidermal atrophy, in contrast to the orthohyperkeratosis and acanthosis seen in lichen planus. The sawtooth appearance of the lower border of the epidermis seen in lichen planus is not a feature of lichen nitidus, and immunofluorescence for immunogloblins is negative. Epithelioid cells and giant cells are characteristic of lichen nitidus and are not typically a feature of lichen planus. Four patients with Crohn disease were reported to develop lichen niditus; however, it remains to be seen if lichen nitidus is truly an extragastrointestinal finding of this disease.39,40 Another patient developed lichen nitidus after hepatitis B vaccine injection.41 The significance of this is uncertain.

Fig. 7.38 Lichen nitidus: numerous tiny papules are present on the chest of a young child. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.

Fig. 7.39 Lichen nitidus: numerous tiny papules are present on the penis. The genitalia are commonly affected. From the collection of the late N.P. Smith, MD, the Institute of Dermatology, London, UK.
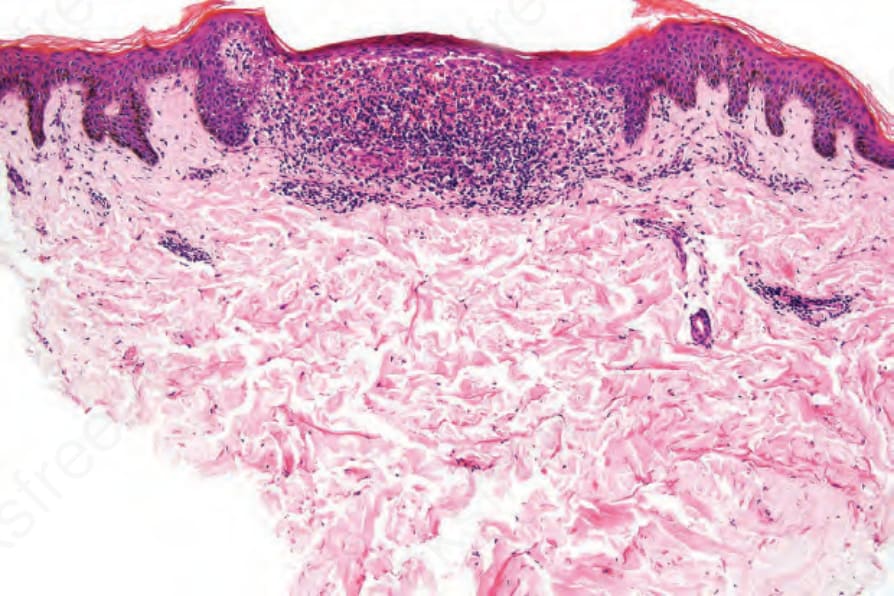
Fig. 7.40 Lichen nitidus: scanning view showing a typical small, circumscribed lesion occupying only a couple of dermal papillae. Note the clawlike epidermal lateral borders.
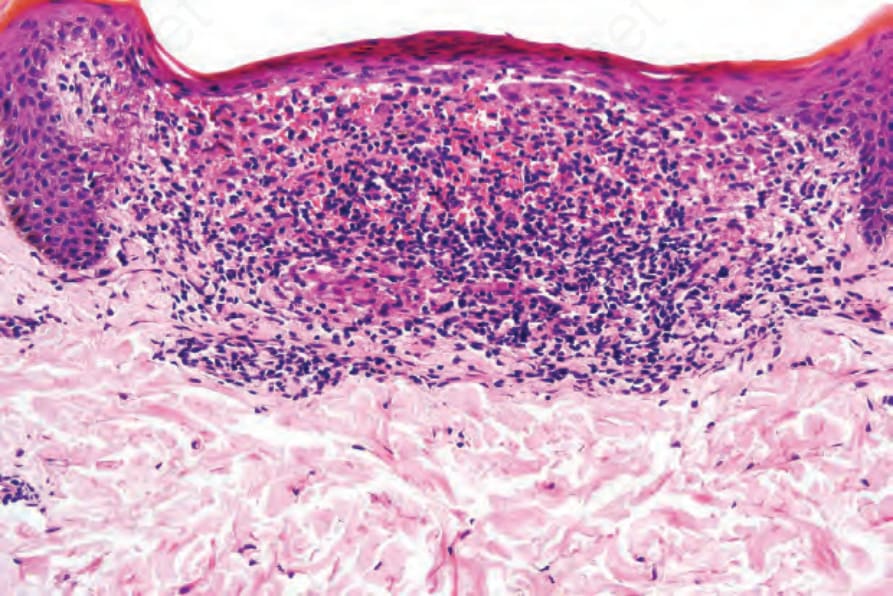
Fig. 7.41 Lichen nitidus: note the parakeratosis and bandlike infiltrate.
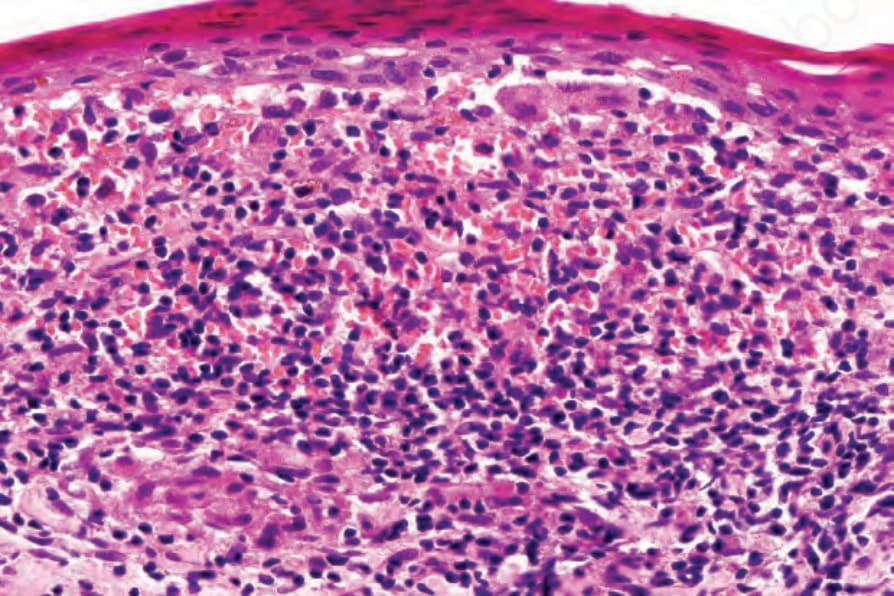
Fig. 7.42 Lichen nitidus: the infiltrate consists of lymphocytes, histiocytes, and epithelioid cells. Ill-defined noncaseating granulomata are not uncommon.
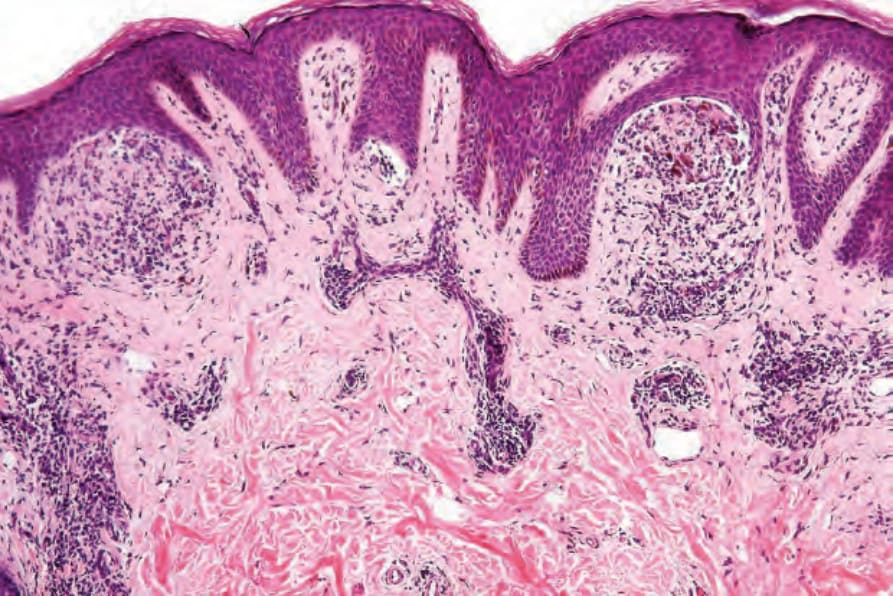
Fig. 7.43 Lichen nitidus: there are multiple lesions of lichen nitidus with an associated granulomatous component. The patient also had typical lichen planus lesions. By courtesy of R. Margolis, MD, St Elizabeth’s Hospital, Boston, USA.
Fig. 7.44 Lichenoid keratosis: there is scaling overlying a slightly raised erythematous plaque. By courtesy of the Institute of Dermatology, London.