Acantholytic acanthoma
Acantholytic acanthoma
Clinical features Acantholytic acanthoma is a common entity consisting of a solitary, usually asymptomatic, keratotic papule or plaque, 0.5–1.5 cm in diameter, often with overlying scale/crust. It usually presents on the trunk, arm, or neck and is clinically thought to be a seborrheic keratosis or actinic keratosis.1–6 A case with central umbilication reminiscent of molluscum contagiosum has also been described.7 Rare examples involving the eyelid have been reported.8 Very occasionally, multiple lesions have been documented.9 Some patients report pruritus. Hemorrhagic bullae may rarely be seen.10 Patients are usually elderly (median age 60 years) and there is a predilection for males (2 : 1).2,4 Lesions are not seen about the head, palms, and soles, and the mucous membranes appear to be spared.2
Pathogenesis and histologic features The pathogenesis of this lesion is unknown. Although one case has been documented in association with immunosuppression, this is likely to be coincidental.11
200 Acantholytic disorders
clinical impression of basal cell carcinoma, actinic keratosis, or squamous cell carcinoma in situ.1,2,3 Rarely, they may present as a subungual lesion.4
Pathogenesis and histologic features The pathogenesis of acantholytic dyskeratotic acanthoma is unknown.
Histologic characteristics include regular epidermal acanthosis showing acantholytic dyskeratosis with grains and corps ronds.1–4 Acantholytic acanthosis is typically confluent, affecting varying levels of the epidermis. Occasionally, it may be confined to the granular and corneal layers or it may be nonconfluent and multifocal.1 Cup-shaped endophytic growth and follicular involvement are not observed.
Differential diagnosis Acantholytic dyskeratotic acanthoma differs from acantholytic acanthoma by the presence of marked dyskeratosis. Focal acantholytic dyskeratosis shows identical histologic features but is an incidental finding rather than a clinically distinct lesion. Warty dyskeratoma is characterized by its cup-shaped and endophytic growth. Pemphigus, Darier disease, and Grover disease differ in their clinical presentation.
Diagnosis is one of exclusion and depends on the solitary nature of the lesion. The histologic features are those of hyperkeratosis, acanthosis, and papillomatosis accompanied by acantholysis affecting all or any layer of the epidermis (Figs 5.80 and 5.81).1 Dyskeratosis may be evident. A perivascular lymphohistiocytic chronic inflammatory cell infiltrate, sometimes with occasional eosinophils, may be present in the superficial dermis.
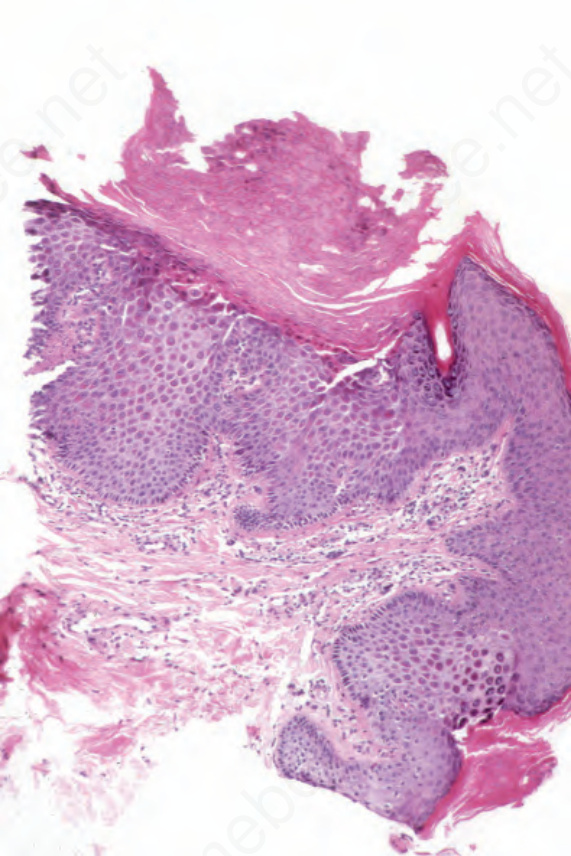
Fig. 5.78 Familial dyskeratotic comedones: this section comes from the edge of a lesion. Note the dell with associated hyperkeratosis and parakeratosis. The acanthosis is in part due to the oblique angle of the cut. By courtesy of B.J. Leppard, MD, Royal South Hants Hospital, UK.
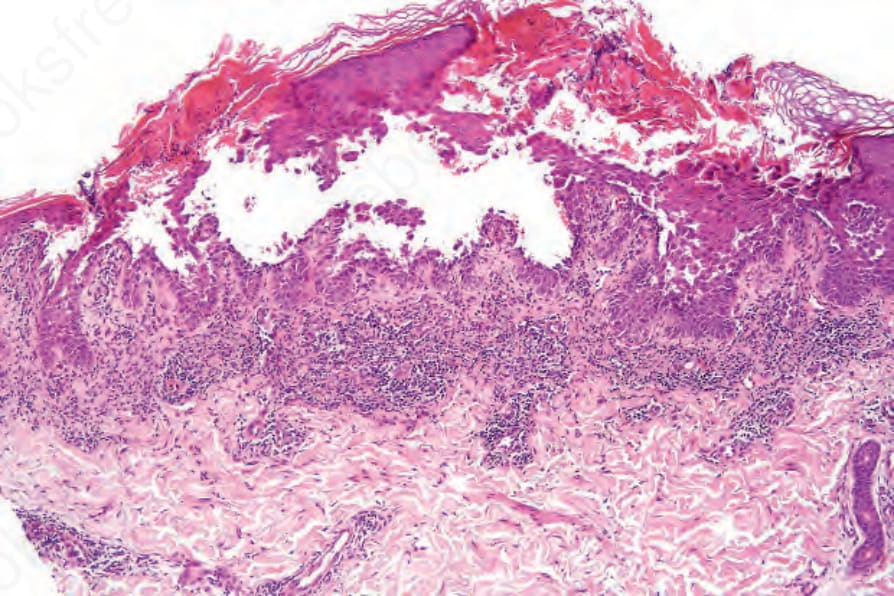
Fig. 5.80 Acantholytic acanthoma: low-power view showing hyperkeratosis, parakeratosis, intraepidermal vesiculation, and multiple foci of acantholysis.
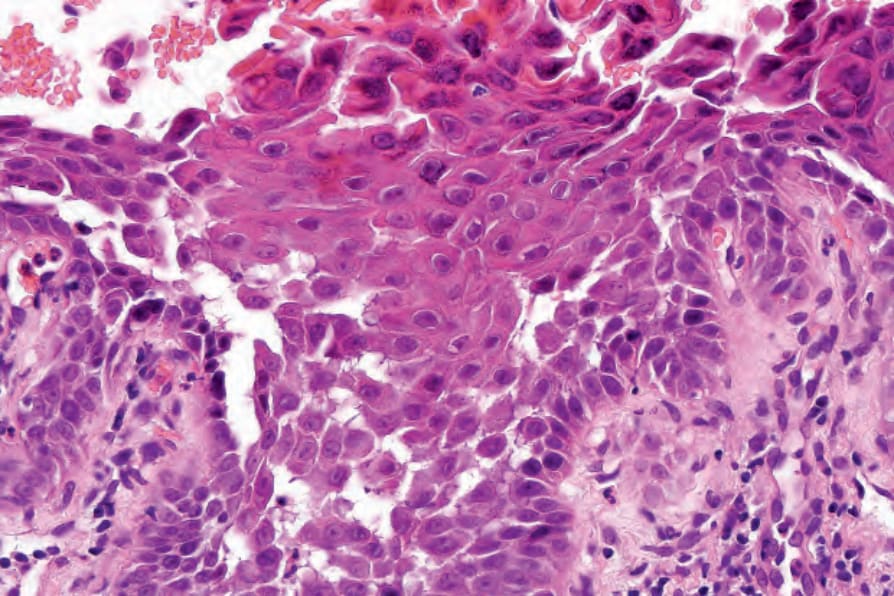
Fig. 5.81 Acantholytic acanthoma: high-power view showing acantholysis and dyskeratosis.
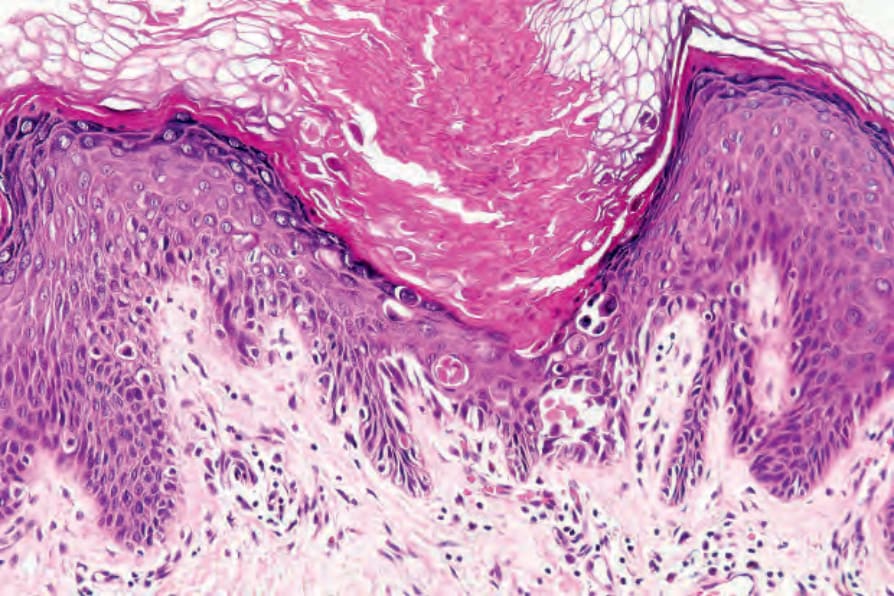
Fig. 5.82 Focal acantholytic dyskeratosis: this example showing the changes of Darier disease was an incidental finding adjacent to a completely unrelated lesion. There was no clinical evidence of Darier disease.