Familial dyskeratotic comedones
Familial dyskeratotic comedones
Clinical features Although thought to be common, familial dyskeratotic comedones have been extremely rarely documented in the literature. To date, only a few families have been reported.1–9 The condition is characterized by an autosomal dominant mode of inheritance. Lesions develop in childhood or adolescence and are permanent.5 Patients present with 1–3-mm-diameter papules containing small hard keratotic plugs, which on removal leave crateriform lesions resembling comedones (Fig. 5.76). Cutaneous horns may also sometimes be apparent (Fig. 5.77).2 Lesions are often generalized but show a predilection for the extremities, particularly the forearms and thighs. The face, scalp, palms, soles, and mucous membranes are typically unaffected. Some patients complain of pruritus or inflammation. There is no evidence of ectodermal dysplasia and systemic lesions are absent.
Histologic features The lesions are characterized by a follicle-like crateriform cystic cavity containing laminated hyperkeratotic and parakeratotic debris and lined by squamous epithelium showing dyskeratosis and sometimes acantholysis at the base (Figs 5.78 and 5.79).4 Grains of Darier are typically present, but corps ronds are sparse and poorly developed. Villi, as seen in Darier disease, are not a feature. Hair shafts and sebaceous glands are absent.
Differential diagnosis The consistent folliculocentric nature of the eruption and absence of nail and oral mucosal changes help distinguish familial dyskeratotic comedones from Darier disease. Corps ronds, a characteristic finding in Darier disease,
199 Acantholytic dermatoses with dyskeratosis
are usually not prominent in familial dyskeratotic comedones. Villus formation and well-developed corps ronds within a solitary lesion distinguish warty dyskeratoma.
Diffuse familial comedones differ by the absence of dyskeratosis.10–13 Familial dyskeratotic comedones may also be mistaken for Kyrle and Flegel diseases:
• Kyrle disease typically presents on the extensor aspect of the lower extremities and presents in adulthood. There is no familial incidence. Histologically, it is characterized by transepidermal elimination of parakeratotic and inflammatory debris. There is no dyskeratosis.
• Flegel disease typically presents in older adults and is characterized by prominent compact hyperkeratosis associated with marked epidermal atrophy, interface change, and dyskeratosis. A keratin-filled crateriform lesion is absent. Perforating folliculitis presents in adults and shows a predilection for the extremities. It is characterized by a crateriform lesion containing a distorted and often curled-up hair shaft.
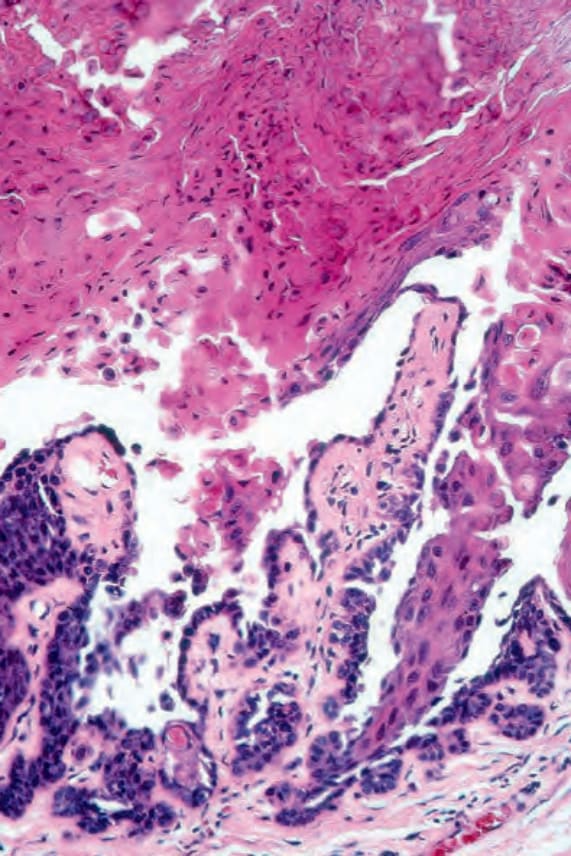
Fig. 5.74 Warty dyskeratoma: note the acantholysis and villi.
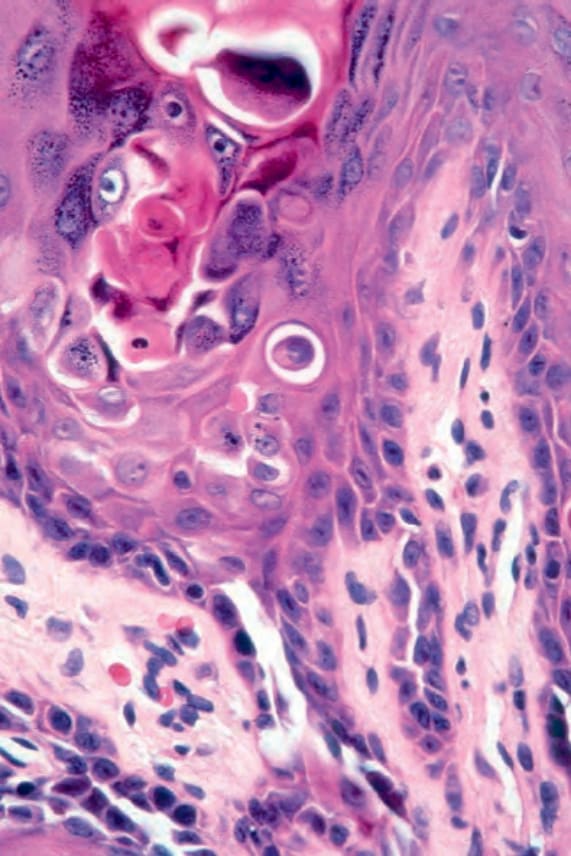
Fig. 5.75 Warty dyskeratoma: corps ronds are conspicuous.

Fig. 5.76 Familial dyskeratotic comedones: numerous comedones are present on the penis and foreskin. By courtesy of B.J. Leppard, MD, Royal South Hants Hospital, UK.

Fig. 5.77 Familial dyskeratotic comedones: a small cutaneous horn is seen arising on the scrotum. By courtesy of B.J. Leppard, MD, Royal South Hants Hospital, UK.
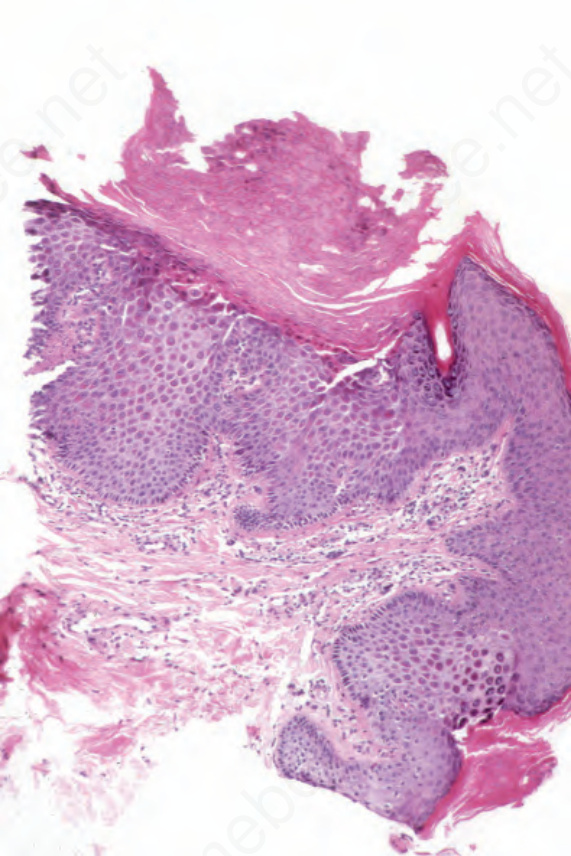
Fig. 5.78 Familial dyskeratotic comedones: this section comes from the edge of a lesion. Note the dell with associated hyperkeratosis and parakeratosis. The acanthosis is in part due to the oblique angle of the cut. By courtesy of B.J. Leppard, MD, Royal South Hants Hospital, UK.
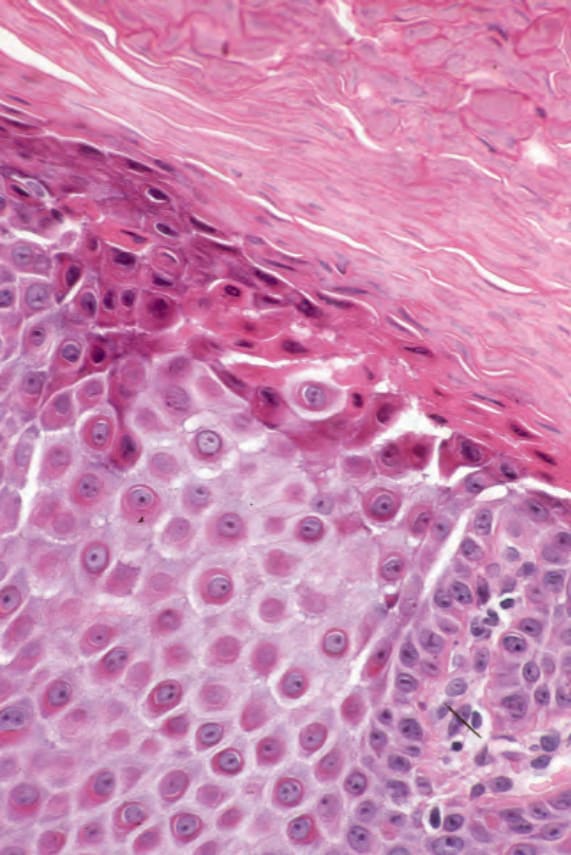
Fig. 5.79 Familial dyskeratotic comedones: note the superficial dyskeratosis. By courtesy of B.J. Leppard, MD, Royal South Hants Hospital, UK