Transient acantholytic dermatosis (Grover disease)
Transient acantholytic dermatosis (Grover disease)
Clinical features Transient acantholytic dermatosis (persistent acantholytic dermatosis) is a primary acquired, self-limiting, acantholytic disease of unknown etiology, seen predominantly in the middle-aged or elderly although there are rare reports of the disorder in children.1–5 Males are affected more often than females (3 : 1).2,3 Light-skinned people are predominantly affected.5 Cases involving blacks are exceptionally rare.6 The disease shows a predilection for the winter months in nonhospitalized patients, although some studies have not shown seasonal variation.7,8 Although the disease is usually transient, persistent and recurring variants have also been described (persistent acantholytic dermatosis) in the literature.9–11 The development of Kaposi varicelliform eruption is a rare and unusual complication of the disease and in one case seems to have been precipitated by vemurafenib.12,13 Occult colonization by herpes simplex virus and S. aureus has also been documented.14,15
The skin lesions are usually rather polymorphic, consisting of 1–3-mm erythematous, red-brown or flesh-colored papules, vesicles, and eczematous plaques with a predilection for the chest, back, and thighs (Figs 5.66 and 5.67).2 Superimposed excoriations are associated with the intensely pruritic eruption. Pustular, bullous, nummular, follicular herpetiform, and zosteriform variants have all been documented.2,16–19 The mucous membranes, palms, and soles are commonly spared although there are rare reports of oral, nasal, and laryngeal involvement.2,20,21 Postinflammatory pigmentary changes following resolution of the acute phase are common. Transient acantholytic dermatosis has been described in association with leukemia and lymphoma in addition carcinoma of kidney, renal pelvis, bladder, and prostate and melanoma.2,22–29 In one study, 25% of patients had some form of malignancy, although that may reflect significant referral bias.24 Other rare associations include scabies, renal failure, peritoneal dialysis, solid organ and bone marrow transplantation, and pregnancy.30–37 It is likely, however, that the majority of these associations are coincidental. Transient acantholytic dermatosis shows a positive correlation with asteatotic eczema, allergic contact dermatitis, and atopic dermatitis.3,38,39
Pathogenesis and histologic features The pathogenesis of Grover disease is incompletely understood. There are, however, a number of important known etiological factors including:
• sun exposure,
• excessive heat and sweating,
• ionizing radiation,
• adverse reaction to drugs. Transient acantholytic dermatosis has long been known to be associated with sun exposure.2,3,40–43 The lesions are photodistributed, and the patients commonly give a history of having recently spent time in the sun.44 There is also a well-established relationship to excessive heat and sweating.43,45–47 Bedridden, febrile patients are particularly at risk and as a result it has been proposed that the pathogenesis might be analogous to that of miliaria. Occlusion of sweat ducts and increased sweating resulting in acantholysis
mediated by high concentrations of sweat urea has been proposed, although this has yet to be proven.48 Immunohistochemistry studies have not generally offered support for this hypothesis, although bedridden, febrile patients may occasionally show prominent involvement of the eccrine duct; this has been termed sudoriferous acrosyringeal acantholytic disease.24,49,50 Associations with sunlamps, sun parlors, PUVA therapy, steam bath, hot tub, hot water bottle, and polyester jogging suits have also been documented.1,2,24 Despite these well-recognized associations, there must be other important predisposing factors, since overexposure to sunlight and excessive sweating are extremely common yet this disease is rare.
Very occasional reports have described transient acantholytic dermatosis developing after radiotherapy for cancer, exceptionally with lesions confined to the area of the port.2,25,51,52 Only a small number of drugs have been
196 Acantholytic disorders
associated (rarely) with the development of transient acantholytic dermatosis.2 There are reports of lesions following treatment with sulfadoxine– pyrimethamine, 2-chlorodeoxyadenosine, D-penicillamine, recombinant interleukin-4, cetuximab, induction chemotherapy for allogeneic bone marrow transplantation, anastrozole, and ipilimumab.53–60 The presence of eosinophils in the dermal inflammatory cell infiltrate has raised the possibility of a hypersensitivity reaction.24 Occasional cases arising in patients with HIV infection have been recorded.24
Despite the histologic similarity to Darier and Hailey-Hailey diseases, there is no evidence of a mutation in the ATP2A2 gene.61
There have been a variety of both direct and indirect immunofluorescence observations including lupus erythematosus-like, bullous pemphigoid-like, and pemphigus-like findings.24,62 These are reviewed in reference 2. A further study has shown autoantibodies in sera from Grover disease patients to a variety of proteins involved keratinocyte development, growth, adhesion, and motility.63 The significance of these findings has not been established. Immunohistochemistry observations have included a reduction or absence of desmosomal staining with cytoplasmic redistribution of the proteins, desmoplakins I and II, plakoglobin, and desmoglein.64–66 Redistribution and dissolution of desmosomal attachment plaques have been demonstrated as the first stage in the development of Grover disease.66 Sera from Grover disease patients has also been shown to decrease expression of Dsg and Dsg3 in experimental models.63
Instead of featuring specific histopathological changes, Grover disease classically mimics three other diseases: Darier disease, Hailey-Hailey disease, and pemphigus (p. vulgaris and p. foliaceus) (Figs 5.68–5.71).24 The first is by far the most commonly encountered. Thus, in the typical case, there is hyperkeratosis, parakeratosis, acanthosis, and acantholysis accompanied by corps ronds formation and grains of Darier. In the Hailey-Hailey pattern, the acantholysis is much more pronounced such that the dilapidated brick wall appearance is seen. Follicular or acrosyringeal involvement may be present.50,67 In a subset of Grover disease, acrosyringeal involvement is quite pronounced and has been termed sudoriferous acrosyringeal acantholytic disease.50 In the pemphigus-like variant, dyskeratosis is typically absent. Multiple specimens from any one patient may disclose differing histologic variants, and superimposed spongiosis is often present. Occasional bullae are encountered, and sometimes this can result in histologic overlap with herpesvirus infection.68 A variable dermal mononuclear infiltrate is usual and significant numbers of eosinophils and/or neutrophils are seen in some cases.21 The earliest changes can consist of elongation of rete ridges with focal acantholysis, mild spongiosis, and a superficial perivascular infiltrate that may be difficult to diagnose as Grover disease.69 Additional features that have been described include porokeratosis-like columns of parakeratosis, lichenoid interface change, reactive keratinocyte atypia, papillary dermal hemorrhage, and epidermolytic hyperkeratosis.70,71
Differential diagnosis Clinically, transient acantholytic dermatosis is easily differentiated from Darier disease, Hailey-Hailey disease, and pemphigus. However, the biopsy findings often mimic these diseases. A histologic clue to the diagnosis is the small size of the lesion. Usually, only one or two small discrete lesions that span a few rete ridges are noted. This is in contrast to other acantholytic dermatoses, which tend to involve the entire biopsy. Biopsies from a patient with Grover disease often show varying features mimicking more than one of the acantholytic dermatoses, and occasionally a number of patterns are seen in a single biopsy specimen. Sometimes, a biopsy will show non-specific features of spongiotic dermatitis. The association of both spongiosis and acantholysis may be a useful pointer to the diagnosis of Grover disease (see also Table 5.2).
197 Acantholytic dermatoses with dyskeratosis

Fig. 5.66 Grover disease: innumerable erythematous papules are present on the chest wall. By courtesy of the Institute of Dermatology, London, UK.

Fig. 5.67 Grover disease: close-up view. By courtesy of the Institute of Dermatology, London, UK.
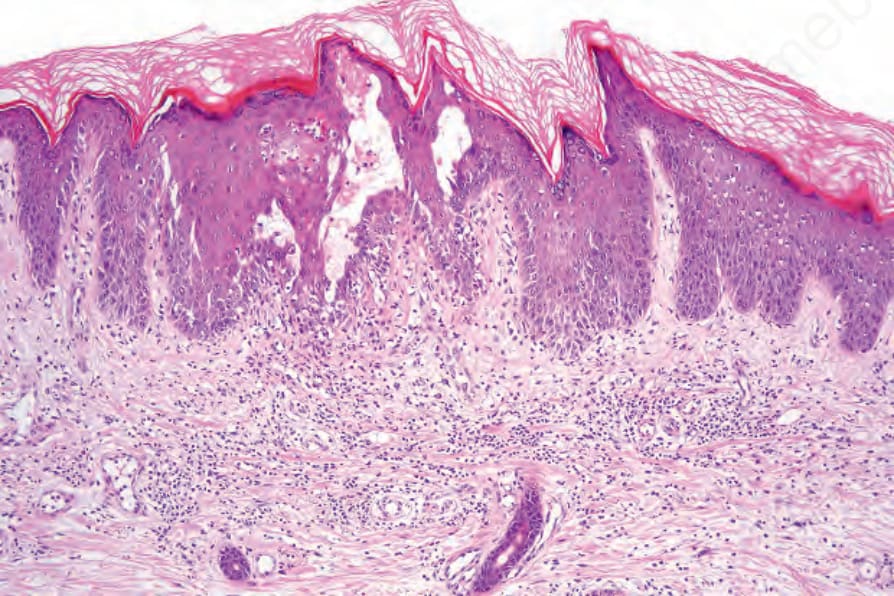
Fig. 5.68 Grover disease: low-power view showing an intact intraepidermal vesicle.
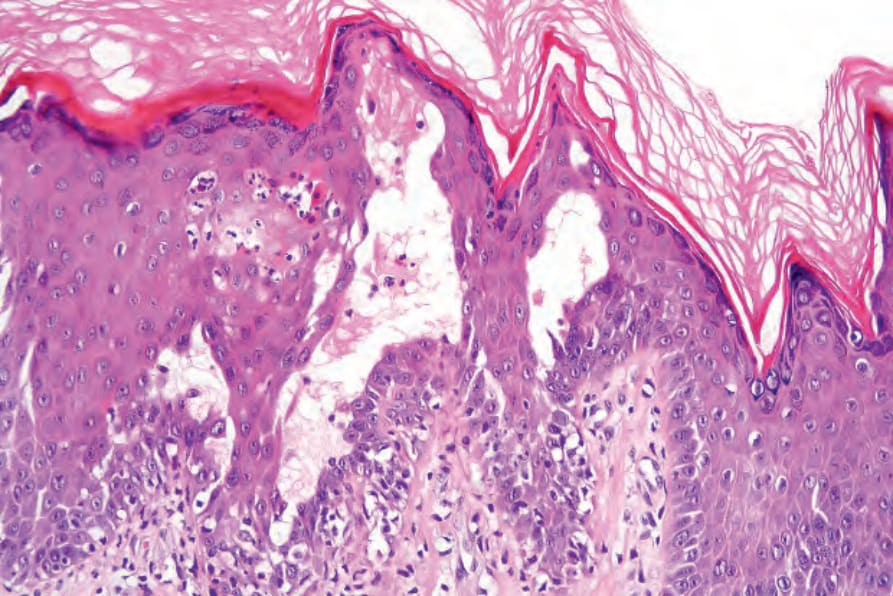
Fig. 5.69 Grover disease: high-power view showing acantholysis.
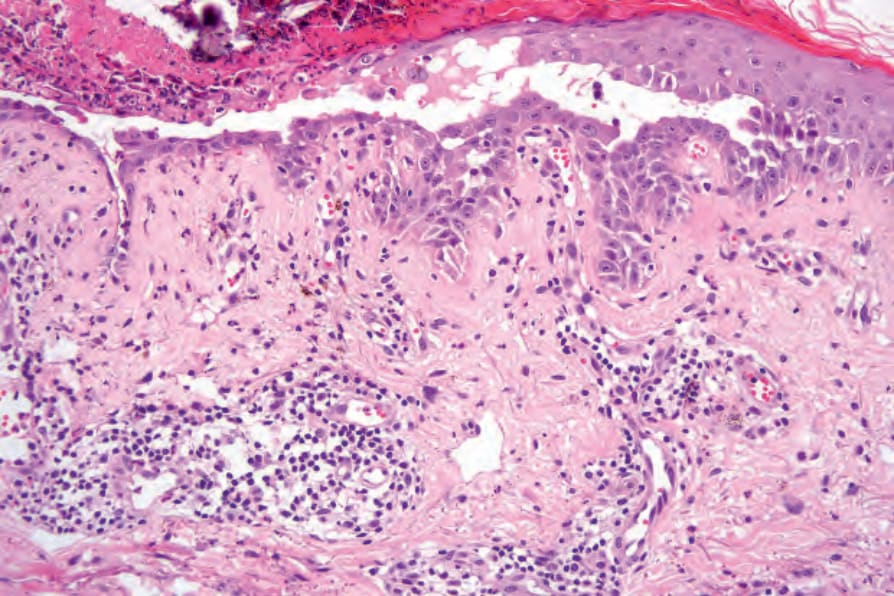
Fig. 5.70 Grover disease: this example is indistinguishable from pemphigus vulgaris.
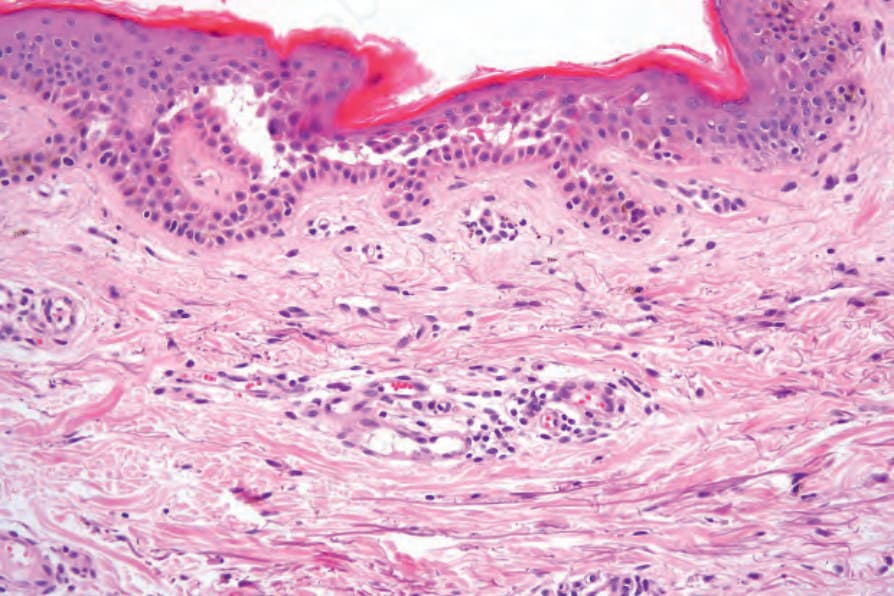
Fig. 5.71 Grover disease: early lesion showing intraepidermal vesiculation.
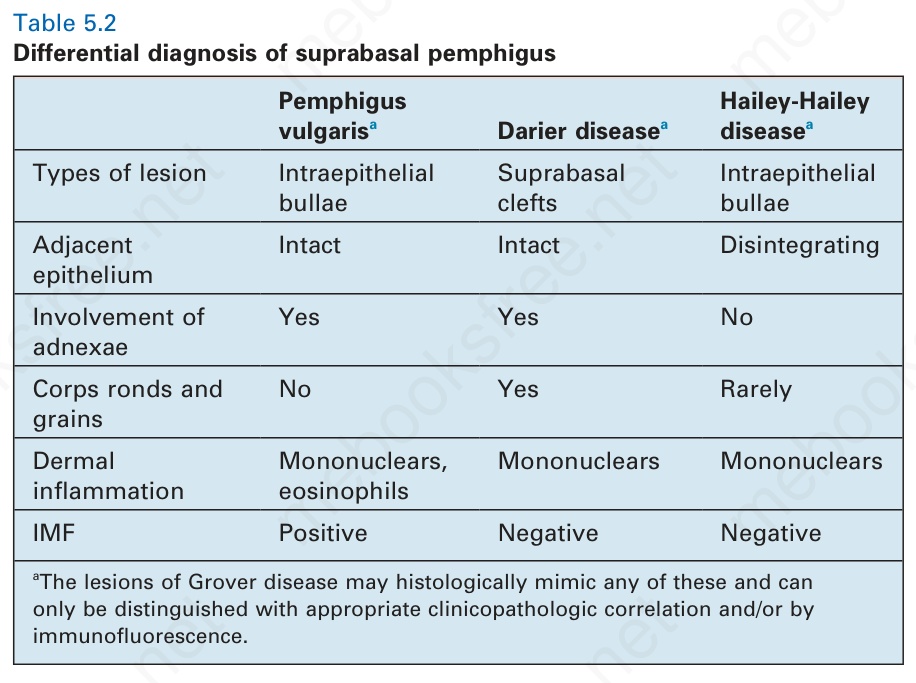
Table 5.2 Differential diagnosis of suprabasal pemphigus