Linear Darier disease
Linear Darier disease
Clinical features Linear Darier disease (acantholytic dyskeratotic epidermal nevus, unilateral Darier disease, zosteriform Darier disease, segmental Darier disease) is a rare acquired condition characterized by the development of grouped, keratotic, sometimes pruritic, yellow-brown papules which affect the trunk, trunk and limbs, limbs, scalp, vulva, and face in decreasing order of frequency (Fig. 5.65).1–9 Their linear distribution corresponds to the lines of Blaschko. Lesions may be aggravated by sunlight, heat, and sweating. Although a wide age range may be affected, the majority of patients are in the third or fourth decade. Both sexes are equally affected. There is no family history of Darier disease. Usually, patients are free from other stigmata of Darier disease, but there are very occasionally reports of patients with linear lesions associated with ipsilateral nail changes and palmar pits typical of Darier disease.10,11
Pathogenesis and histologic features The precise nature of this lesion remains conjectural. Although many authors prefer to regard it as a variant of epidermal nevus with superimposed acantholytic dyskeratosis, there is an alternative school of thought which believes that many, if not all, such lesions represent localized or unilateral Darier disease, arguing that the condition develops as a consequence of genetic mosaicism. Certainly, the late age of onset is unlike a typical epidermal nevus, which usually presents in childhood. The distribution along
the lines of Blaschko and the occasional reports of additional Darier-like features on the ipsilateral side of the body offers support to a concept of localized Darier disease. Recently, ATP2A2 mutations have been identified in lesional tissue but not unaffected skin patients with linear acantholytic epidermal nevi, confirming the relationship of these lesions to Darier disease.12,13,14
Histologically, these lesions are indistinguishable from Darier disease.
Differential diagnosis Very rarely, true epidermal nevus may show histologic features of acantholysis and dyskeratosis presenting against a background of a verrucous plaque characterized by marked acanthosis and papillomatosis.15,16 Such lesions, which are present at birth, would be best classified as epidermal nevus showing acantholysis and dyskeratosis rather than being included in the spectrum of acantholytic dyskeratotic epidermal nevus.
195 Acantholytic dermatoses with dyskeratosis
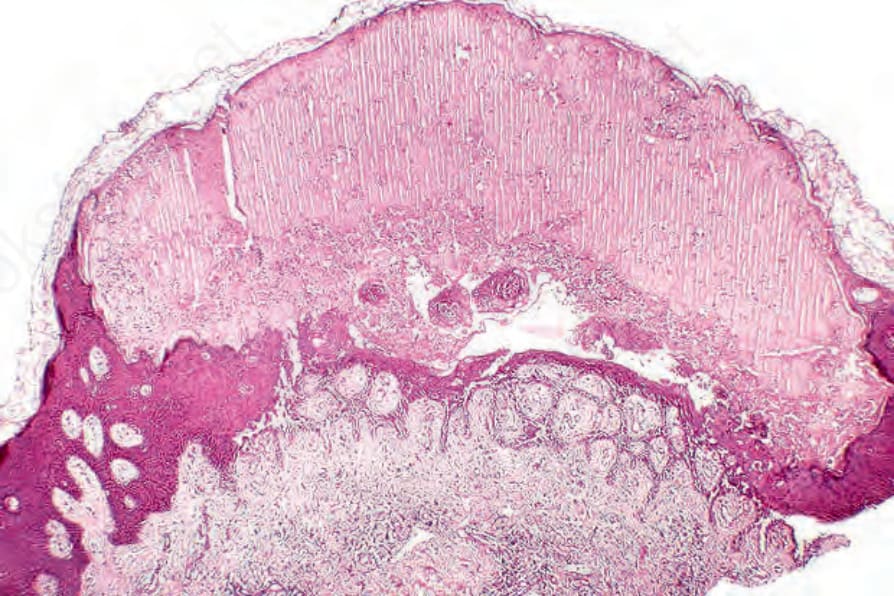
Fig. 5.63 Darier disease: bullous variant showing suprabasal acantholysis, epidermal regeneration, and a subcorneal blister.
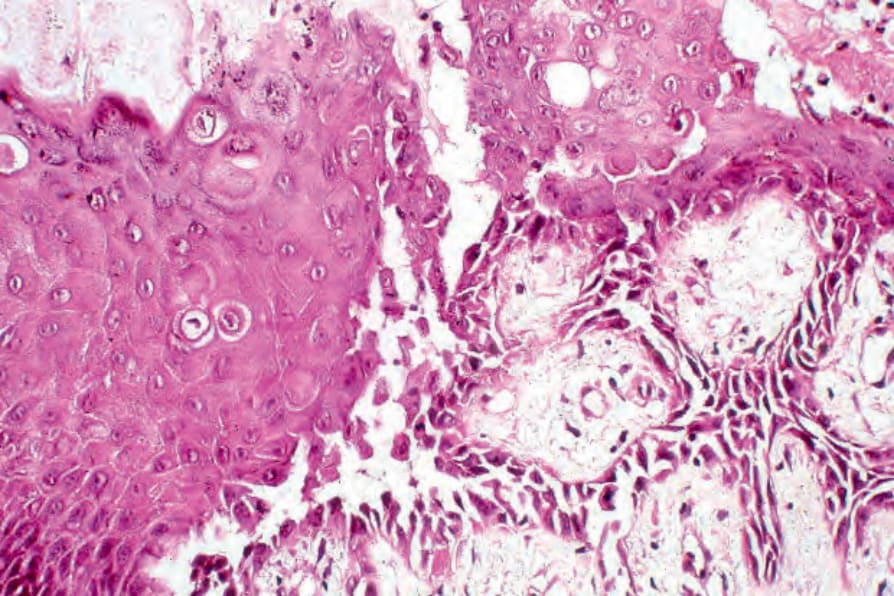
Fig. 5.64 Darier disease: high-power view of Fig. 5.62 showing multiple corps ronds.

Fig. 5.65 Linear Darier disease: the trunk is a commonly affected site. Note the small papules. Courtesy of the Institute of Dermatology, London, UK.