Darier disease
Darier disease
Clinical features Darier disease (keratosis follicularis, morbus Darier), which is characterized by abnormal keratinocyte adhesion, is a rare hereditary disorder, usually transmitted in an autosomal dominant pattern. In a large series, however, 47% of patients had no clear family history of Darier disease.1 Presumably, these cases represent new mutations or evidence of incomplete penetrance. Its documented incidence is variable. In Oxfordshire (UK), the incidence is 1 : 55 000, in the north of England it is 1 : 36 000, in the west of Scotland it is 1 : 30 000, whereas in Denmark it is 1 : 100 000.2–5 The sex incidence is equal, although males appear to be more severely affected than females. The disease usually presents in the first or second decade (with a peak around puberty) and often follows exposure to ultraviolet light.1 Exceptionally, patients may not present until their sixth or seventh decade.6 Darier disease is a long-term illness. Remissions do not occur, although some patients show improvement with increasing age.6
The lesions are frequently itchy and, less commonly, painful.1,6,7 They are characterized by greasy, crusted, keratotic yellow-brown papules and plaques found particularly on the ‘seborrheic’ areas of the body – the scalp, forehead, ears, nasolabial folds, upper chest, back, and supraclavicular fossae (Figs 5.49–5.53).1,5,7 There is mild involvement of the flexures in the majority of patients although sometimes this distribution predominates.1,6,7 Lesions may be induced or exacerbated by stress, heat, sweating, and maceration.1,7,8 In some areas, the lesions have a warty appearance, whereas in
191 Acantholytic dermatoses with dyskeratosis
the flexures they are often vegetative, malodorous (a particularly distressing problem), and often secondarily infected (Figs 5.54 and 5.55).6,7 Bullous lesions generally following sun exposure can occur, albeit rarely.9–12 Leukodermic macules in black patients have also been described and in the absence of more clinical typical changes of the disease, the diagnosis may be very difficult.13–16 Additional features including cutaneous horns and hemorrhagic acrallesions have also been documented.17–22
Patients with Darier disease are susceptible to bacterial (particularly S. aureus), dermatophyte, Candida, and viral infections.1,19,20,23–26 There are rare case reports of eczema vaccinatum and eczema herpeticum complicating Darier disease, and patients who developed localized anogenital and disseminated cowpox have also been reported.27–30 Life-threatening Kaposi varicelliform eruption is a rare but important complication that is seen in severely affected patients and is usually associated with herpes simplex virus
superinfection.31–34 No consistent abnormality of immune function has been found to explain this.35,36 Recently, however, persistence of intracellular S. aureus small-colony variants in a patient with Darier disease has been shown to be of importance in chronic cutaneous infection and resistance to antibiotic therapy.37 Lesional skin is also frequently colonized by S. aureus, and disease severity is correlated with extent of colonization.26 Other cutaneous manifestations of Darier disease include unilateral, linear, or zosteriform variants, which some regard as acantholytic, dyskeratotic epidermal nevi rather than true Darier disease (see below).38,39 It is more likely that these variants, at least in part, result from genetic mosaicism, and there is molecular evidence supporting this view.40–42
The hands are affected in 96% of patients.1 Pits and punctate keratoses with focal disruptions of the skin ridges of the palms and soles are
192 Acantholytic disorders
50% of patients and consist of small white papules on the hard palate.55,57,58 Large nodular and verrucous plaques are also sometimes present, and occasionally there are gingival, buccal mucosal, and tongue lesions.17,56 Involvement of the salivary ducts results in salivary gland swelling with obstruction and sialadenitis.59,60 Involvement of the parotid gland can be seen in up to 30% of cases.57 Anal involvement may present as pruritus ani or less often as vegetating malodorous plaques.61
Ocular lesions, particularly affecting the cornea, are seen in up to 76% of patients.62 Peripheral corneal opacities and central epithelial irregularity are the usual findings. Pannus formation may rarely be present. Lesions are typically asymptomatic.
Associated systemic abnormalities are unusual, but include epilepsy, pulmonary lesions, bone cysts, low intelligence, and small stature.1 Various neuropsychiatric problems including depression and bipolar disorder have been linked with Darier disease.6,63–65 There is some evidence to suggest that there is familial cosegregation of bipolar disorder with Darier disease, at least in a proportion of cases.63,64
Rare and likely incidental associations include visceral malignancy, horseshoe kidney, hemodialysis, gynecomastia, cutis verticis gyrate, and Fanconi anemia.66–71
characteristic features (Fig. 5.56).1,6,43 Acrokeratosis verruciformis-like lesions are common on the backs of the hands.1 Indeed, acrokeratosis verruciformis of Hopf, a localized disorder of keratinization of distal extremities, is closely related to Darier disease and appears to be caused by mutations in the same gene.44,45
Nail changes are a particularly important diagnostic feature.1,2,6,46–48 Longitudinal white or red streaks (often both), some of which terminate in a small nick on the free margin, are typical findings (Figs 5.57 and 5.58).1,48 Painful splitting and subungual hyperkeratoses are additional manifestations.1 The toenails are affected less often (and less severely) than the fingernails.1 Subtle hand and nail manifestations may sometimes be a presenting feature.6
The mucous membranes of the mouth, pharynx, larynx, esophagus, and female genitalia can also be affected.49–58 Oral lesions are present in up to
Spontaneous remissions in Darier disease are rare, and in the majority of patients the disease persists throughout life.
Pathogenesis and histologic features Positional cloning studies of different families have all shown the gene of Darier disease to be located at 12q23-q24.72,73 Mutations in ATP2A2, a gene that encodes for SERCA2 (type 2 sarcoendoplasmic reticulum CA2+-ATPase), cause the disease and have been identified in the majority of patients screened.73 So far, over 100 different mutations have been reported, with new novel mutations constantly being reported. They are predominantly missense mutations, but frameshift and splice site mutations as well as mutations resulting in a premature stop codon have also been identified.74–87 However, no clear genotype–phenotype correlation has emerged. The disease is likely a result of haploinsufficiency since only one correct copy of the ATP2A2 gene is expressed.88 The mutant copy may furthermore lead to enhanced proteasome-mediated degradation and/or
protein dimerization resulting in complete loss of SERCA2 activity.88,89 The precise mechanism of how mutations in the ATP2A2 gene lead to disease is unknown although there is emerging evidence to suggest that the integrity of intercellular junctions is dependent on the intracellular calcium stores.90 SERCA is a ubiquitously expressed calcium-ATPase, and its function is the transport of cytosolic calcium ions into the endoplasmic reticulum.88 There are three different genes encoding these proteins, resulting in a total of nine different isoforms. Of the different isoforms, only SERCA2b appears to be expressed in keratinocytes.91 Loss of SERCA2 function can therefore not be compensated for, explaining the severe skin manifestations in the absence of further systemic involvement in most patients with Darier disease.88 Ultimately, intact intracellular calcium ion homeostasis has been identified as a major factor in the complex process of desmosome assembly and is necessary for intracellular interactions between desmosomal cadherins and intracellular plaque proteins such as plakoglobin.88,92 Apoptosis in Darier disease resulting in dyskeratotic cells is likely directly related to the imbalance in calcium homeostasis, and immunohistochemical studies have revealed reduced expression of antiapoptotic proteins of the bcl-2 gene family in lesional epidermis.93–95 It has recently been shown that mutant SERCA2 accumulates as insoluble aggregates resulting in endoplasmic resticulum stress and induction of apoptosis.96
193 Acantholytic dermatoses with dyskeratosis
No single specific ultrastructural abnormality has been identified in Darier disease. Changes described have included complete loss of desmosomes in foci of acantholysis with formation of cell membrane microvilli, cytoplasmic vacuolization, cell membrane defects, abnormal tonofilament aggregation, clumping and distribution, premature and abnormal formation of keratohyalin granules and membrane coating (Odland) bodies, and excessive lipid lamellae between the flattened keratinocytes of the stratum corneum.97–101 Hemidesmosomes and the lamina densa usually appear morphologically normal, although discontinuities of the latter have been described. Ultrastructurally, corps ronds are characterized by large dense keratohyalin masses, numerous membrane coating granules, and tonofilament clumps.97 They are distributed particularly around the nucleus, often surrounding a perinuclear cytoplasmic halo containing distended vesicles. Grains of Darier are composed of nuclear remnants with surrounding dyskeratotic debris.97
Acantholysis develops as a consequence of desmosomal breakdown and dissociation of tonofilaments, although which comes first is uncertain.
The histologic features of Darier disease depend on a variable interplay between acantholysis and abnormal keratinization (dyskeratosis), the acantholysis resulting in suprabasal cleft formation (and rarely vesicles or even blisters), and the dyskeratosis manifesting as corps ronds and grains of Darier.
• Corps ronds are large structures, usually most conspicuous in the granular layer, and consist of an irregular eccentric and sometimes pyknotic nucleus surrounded by a clear halo enclosed within a basophilic or eosinophilic ‘shell’ (Fig. 5.59). Variable amounts of highly irregular keratohyalin granules may also be evident.
• Grains are located within the horny layer and consist of somewhat flattened oval cells with elongated cigar-shaped nuclei and abundant keratohyalin granules. In the fully established lesion, there is hyperkeratosis and often parakeratosis, sometimes arranged in a clearly defined tier (Figs 5.60–5.62). The epidermis may appear acanthotic or atrophic and typically shows acantholysis with suprabasal cleft formation in which the underlying dermal papillae, covered by a single layer of epithelium, project into the cavity (villus formation). The roof contains variable numbers of grains, and the adjacent epithelium has variable numbers of corps ronds. Occasionally, epithelial proliferation can be marked, resulting in pseudoepitheliomatous hyperplasia. Bullous lesions are illustrated in Figs 5.63 and 5.64.
There may be a perivascular chronic inflammatory cell infiltrate in the superficial dermis, although this is not a common finding.
The histologic features of the oral, pharyngeal, laryngeal, and esophageal lesions are similar to those described in the skin although dyskeratosis is said to be less conspicuous.57 Salivary gland lesions show ductal dilatation and squamous metaplasia of the lining epithelium with acantholysis and dyskeratosis.59,60
194 Acantholytic disorders
Corneal lesions are characterized by corneal epithelial edema, subepithelial granular deposits, and basement membrane thickening. Acantholysis and dyskeratosis are not seen.47
Differential diagnosis Although warty dyskeratoma, Hailey-Hailey disease, and pemphigus are considered in the differential diagnosis of Darier disease, their distinction is not challenging when clinical information is considered. Warty dyskeratoma is a single umbilicated lesion that typically forms more pronounced papillary structures. Hailey-Hailey disease is characterized by full-thickness epidermal acantholysis and does not show extensive dyskeratosis. Grover disease may be indistinguishable from Darier disease in a given biopsy, but the lesions are usually small, spanning only a few rete ridges. The presence of some combination of spongiosis, and changes mimicking more than one of the acantholytic dermatoses, is characteristic of Grover disease. In cases that show only Darier-like changes, clinical information should allow for definitive diagnosis.

Fig. 5.49 Darier disease: in this patient, keratotic brown papules are present on the back of the neck. From the slide collection of the late N.P. Smith, MD, the Institute of Dermatology, London, UK.

Fig. 5.50 Darier disease: close-up view of keratotic papules. From the slide collection of the late N.P. Smith, MD, the Institute of Dermatology, London, UK.

Fig. 5.51 Darier disease: this patient shows a striking symmetrical distribution. From the slide collection of the late N.P. Smith, MD, the Institute of Dermatology, London, UK.

Fig. 5.52 Darier disease: lesions may be induced by heat, sweating, and maceration. From the slide collection of the late N.P. Smith, MD, the Institute of Dermatology, London, UK.

Fig. 5.53 Darier disease: close-up view. From the slide collection of the late N.P. Smith, MD, the Institute of Dermatology, London, UK.

Fig. 5.54 Darier disease: skin involvement as severe as this is fortunately extremely rare. By courtesy of M. Greaves, MD, the Institute of Dermatology, London, UK.
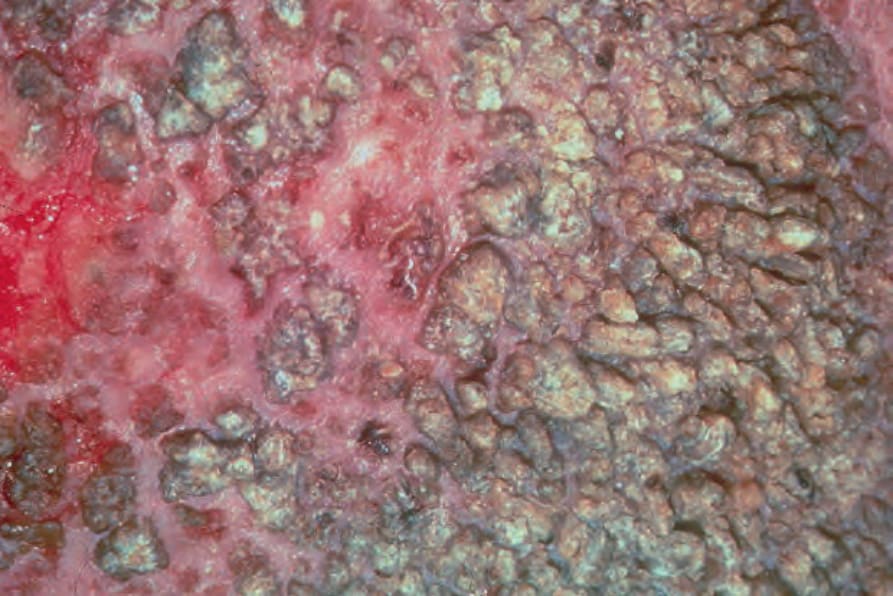
Fig. 5.55 Darier disease: severe involvement can be very disfiguring and a source of considerable disability and embarrassment. By courtesy of M. Greaves, MD, the Institute of Dermatology, London, UK.

Fig. 5.56 Darier disease: palmar pits are a helpful diagnostic clue. By courtesy of J. Wilkinson, MD, Wycombe General Hospital, High Wycombe, UK.

Fig. 5.57 Darier disease: parallel white and red longitudinal streaks are pathognomonic features. By courtesy of the Institute of Dermatology, London, UK.

Fig. 5.58 Darier disease: notches on the free margin of the nail are common findings. By courtesy of the Institute of Dermatology, London, UK.
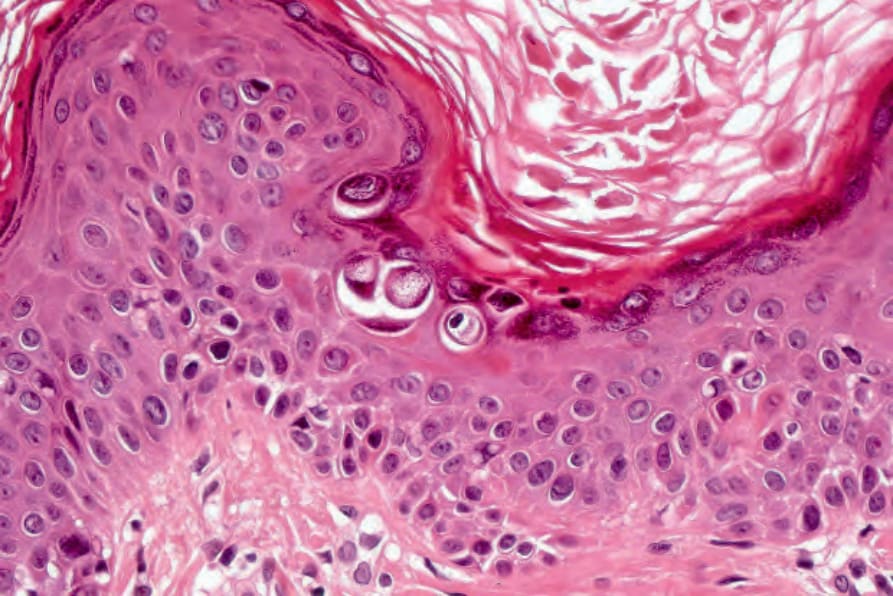
Fig. 5.59 Darier disease: very early lesion showing multiple characteristic corps ronds.
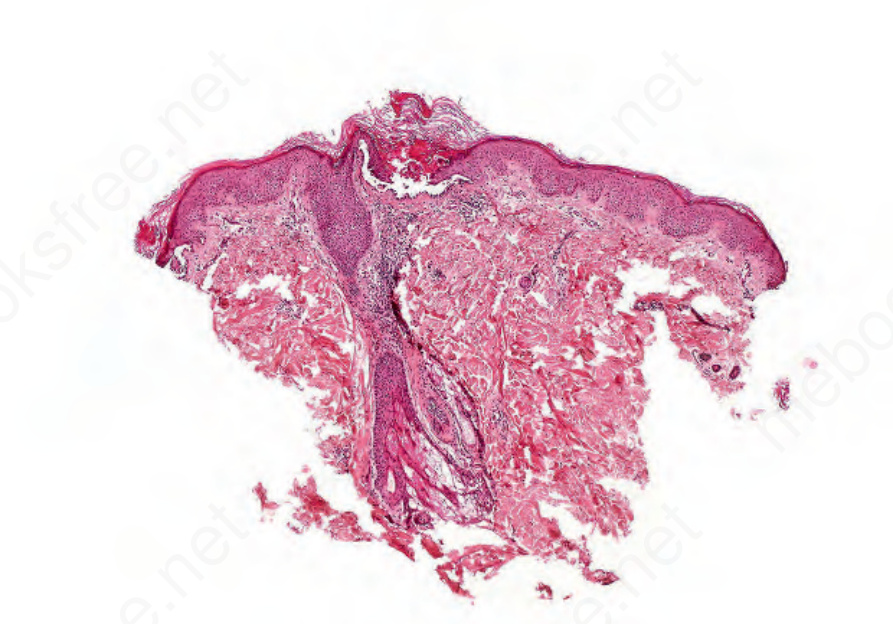
Fig. 5.60 Darier disease: scanning view through a typical lesion. Note the keratotic tier and suprabasal cleft formation.
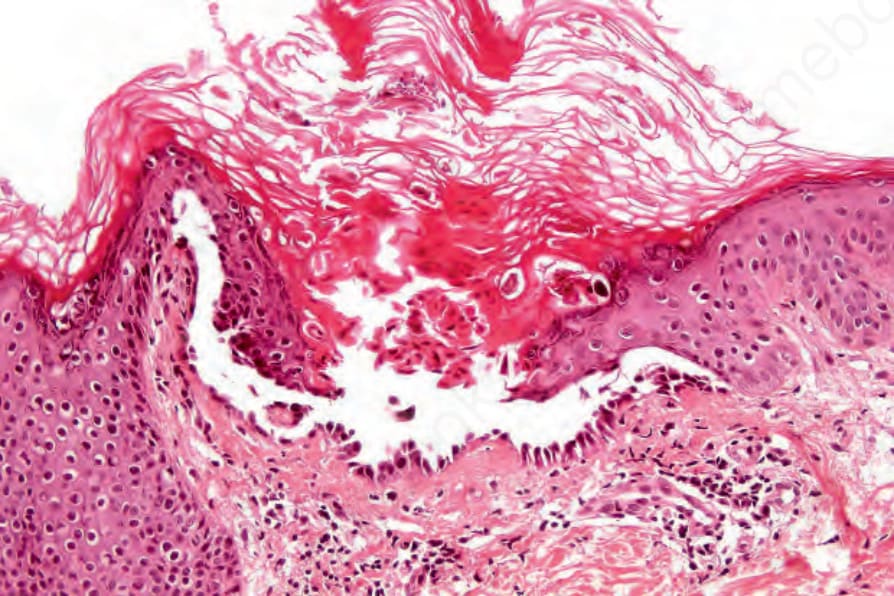
Fig. 5.61 Darier disease: higher-power view showing the well-developed vesicle with suprabasal acantholysis and well-developed corps ronds and grains.
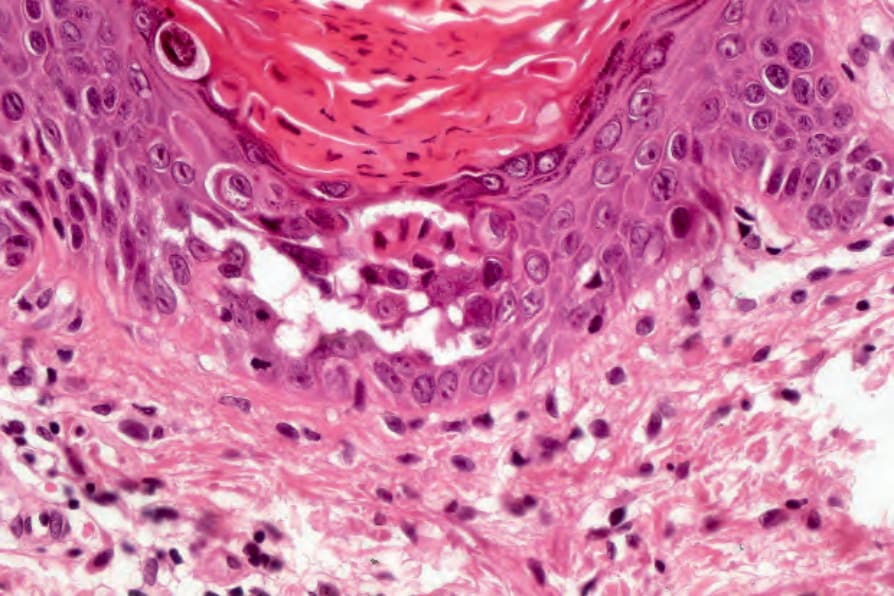
Fig. 5.62 Darier disease: in this example, both corps ronds and grain of Darier are evident.
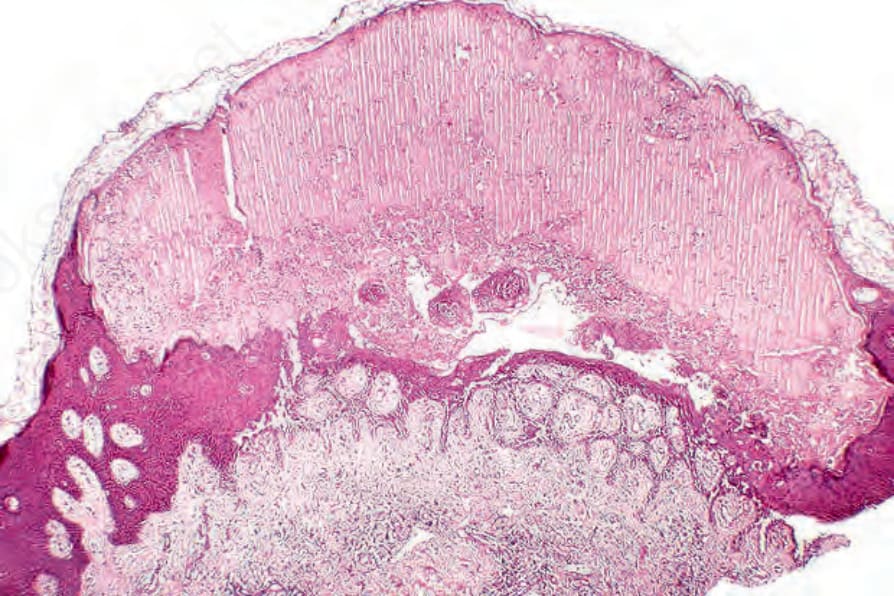
Fig. 5.63 Darier disease: bullous variant showing suprabasal acantholysis, epidermal regeneration, and a subcorneal blister.