Hailey-Hailey disease
Hailey-Hailey disease
Clinical features
Hailey-Hailey disease (benign familial pemphigus) is a rare, episodic, acantholytic disorder with an autosomal dominant mode of inheritance.1,2 In only about two-thirds of patients, however, is a family history obtained. There is an equal sex incidence.2,3
Significant associated conditions have not been documented with the possible exception of a bipolar disorder and a patient with affective disorder (see Darier disease).35,36 An association with supernumerary nipples has been documented in one Tunisian family.37
Exceptionally, squamous carcinoma has been documented as a complication in patients with Hailey-Hailey disease.38,39 It is likely, however, that those arising on the vulva have a human papillomavirus-associated basis.40,41 Condylomatous change and evidence of HPV infection has recently been detected in genital lesions of the disease.42,43 Two patients with Hailiey-Hailey disease and multiple primary melanomas and other malignancies have been described.44
Lesions usually present in the second to fourth decades and appear particularly at sites of minor trauma or friction, especially flexural, around the neck, and in the axillae and groin (Fig. 5.43).1–4 However, other sites, such as the genitalia, umbilicus, inframammary regions, and scalp, may also be affected. Rarely, the disease may be generalized.5–8 Nikolsky sign is sometimes positive.3 Vesicles and bullae, arising on normal or erythematous skin, are soon replaced by erosions, crusting, and scaly plaques sometimes resembling impetigo (Figs 5.44 and 5.45).2,4,9 Healing is accompanied by hyperpigmentation, but scarring is not a feature.3,4 Lesions are frequently itchy and malodorous. Sometimes pain is a considerable problem, particularly if fissuring is present.3 Symptoms often improve with advancing age.1 Superinfection by Candida albicans, herpes simplex virus, and Staphylococcus aureus are frequent complications.10–13 Segmental involvement has rarely been reported as a result of type 1 or type 2 mosaicism according to the classification by Happle, and it has now become clear that at least some of the cases of relapsing linear acantholytic dermatosis represent type 2 segmental Hailey-Hailey disease.14–19
The development of the lesions is related to mechanical trauma, stress, and ultraviolet radiation, and exacerbation of the disease has been reported due to scabies, contact irritation, patch testing, and multiple pregnancies.20–25
Although it has rarely been reported that Darier disease may coexist with Hailey-Hailey disease, the available evidence supports the contention that these two conditions represent completely different entities.45
Pathogenesis and histologic features Hailey-Hailey disease is primarily an abnormality of cell adhesion. Development of this disease has been shown to be caused by multiple mutations in ATP2C1 on chromosome 3q21–24, a gene that encodes the calcium pump SPCA1 (type 1 sarcoendoplasmic reticulum CA2+-ATPase).46,47 SPCA1 is a Ca2+/Mn2+ ATPase present within the membrane of the Golgi apparatus and responsible for the transport of Mn2+ as well as Ca2+ ions into the Golgi.48,49 Over 100 mutations have been identified spanning the entire ATP2C1 gene including missense, frameshift, splice site, as well as nonsense mutations.5–64 However, no clear genotype–phenotype correlation has emerged as yet. Studies have shown that calcium regulation in cultured keratinocytes is impaired.46 In addition, there is evidence that integrity of intercellular junctions may be dependent on intracellular calcium stores.65–69 The precise mechanism by which the abnormality in the calcium pump causes acantholysis is not known. However, the addition of calcium to monolayers of squamous cells in culture elicits stratification.66 In contrast, cells grown in low calcium medium fail to stratify.68 It should be noted that Darier disease, another disorder showing acantholysis, is also associated with a mutation in another calcium pump – ATP2A2. That both of these disorders of acantholysis are associated with mutations in a calcium pump is strong evidence for an important role in maintaining cell–cell cohesion.
189 Acantholytic dermatoses with dyskeratosis
Immunohistochemical studies have confirmed that the major desmosomal proteins and glycoproteins are synthesized in Hailey-Hailey disease and distributed along the plasma membranes in uninvolved epidermis.70 In lesional skin, there is marked cytoplasmic labeling for the desmoplakins (DpI, DpII), desmogleins (Dsg2, Dsg3), and desmocollins.70–74 Studies on keratinocyte differentiation demonstrate premature expression and reduced levels of involucrin due to increased mRNA degradation, and it has been proposed that intact ATP2C1 is necessary for basal cell layer keratinocytes to maintain their undifferentiated state.75,76 A number of interesting observations have been made recently in both Hailey-Hailey disease and Darier disease that provide further insight into how the alteration in the calcium gradient affects ATP receptors and keratin expression.77 In both diseases, there is a lower level of calcium in the basal cell layer of the epidermis compared to normal skin; the ATP receptor P2Y2 is not identified at the cellular membrane in affected cells whereas P2X27, which is usually not present on the cellular membrane, is expressed in these cells probably mediating apoptosis. Furthermore, both keratins 14 and 10 are expressed in diseased cells whereas these keratins are mutually exclusive in normal keratinocytes.
While early lesions show suprabasilar lacunae, established Hailey-Hailey disease is characterized by massive acantholysis associated with suprabasal vesicle or bulla formation.3 Typically, however, the acantholysis is incomplete, with the cell retaining some connections and giving an appearance often likened to a ‘dilapidated brick wall’ (Figs 5.46–5.48). The adnexal epithelium is usually spared. Occasionally, dyskeratotic cells resembling corps ronds and grains of Darier disease are seen.
Ultrastructural studies have primarily disclosed abnormalities of the desmosome–tonofilament units, characterized by diminished numbers of desmosomes and clumped tonofilaments.78–81 The latter have a linear distribution in the basal keratinocytes, but develop a whorled configuration in the suprabasal layers.79,81 The cell membranes show microvillus formation.78 An electron microscopic study of artificially induced early lesions suggests the desmosomal splitting precedes the tonofilament clumping.80 Dyskeratotic cells are characterized by condensed tonofilaments surrounding pyknotic nuclei.
disease tends to show prominent suprabasal cleft formation with involvement of adnexae and is associated with numerous corps ronds and grains. These points of distinction are summarized in Table 5.2.
Immunofluorescence studies for immunoglobulin and complement are invariably negative, aiding in the distinction from immunobullous disorders. Distinction from acantholytic dermatosis of the genital area can, however, be extremely difficult. In fact, the relationship between these disorders is not well understood. The combination of clinical features of a lesion or lesions localized to the vulvogenital area and a negative family history favors acantholytic dermatosis of the genital area.
Differential diagnosis The histologic features of Hailey-Hailey disease must be distinguished from those of Darier disease, p. vulgaris, and Grover disease. Pemphigus is distinguished from Hailey-Hailey disease by the presence of relatively intact epithelium in the adjacent epidermis (versus disintegrating ‘dilapidated brick wall’) and involvement of adnexal structures. In difficult cases, positive immunofluorescence staining supports a diagnosis of pemphigus. Darier

Fig. 5.43 Hailey-Hailey disease: erythematous and scaly lesions are present in the groin and on the labia majora. From the slide collection of the late N.P. Smith, MD, the Institute of Dermatology, London, UK.

Fig. 5.44 Hailey-Hailey disease: lesions are most often seen in the flexures as a consequence of friction. By courtesy of the Institute of Dermatology, London, UK.
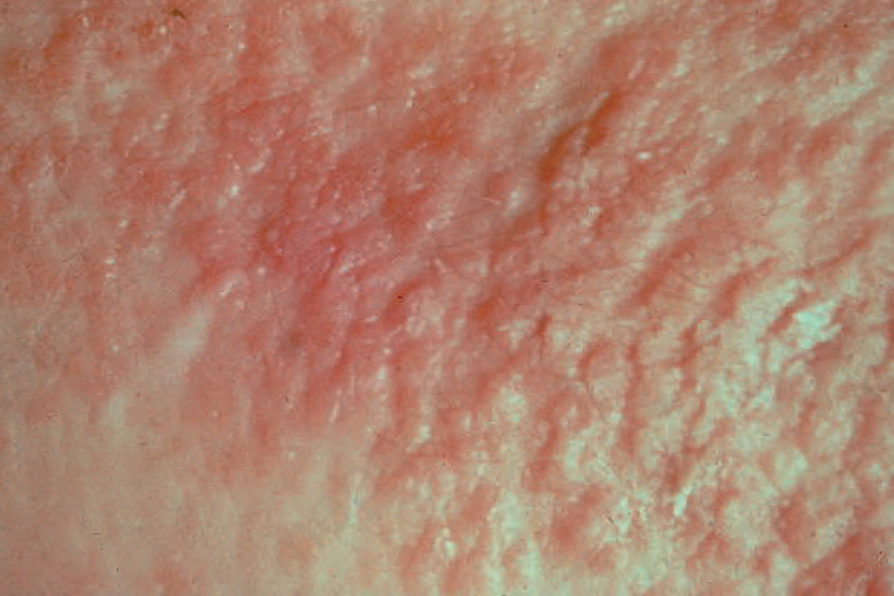
Fig. 5.45 Hailey-Hailey disease: close-up view of keratotic warty lesions. By courtesy of the Institute of Dermatology, London, UK.
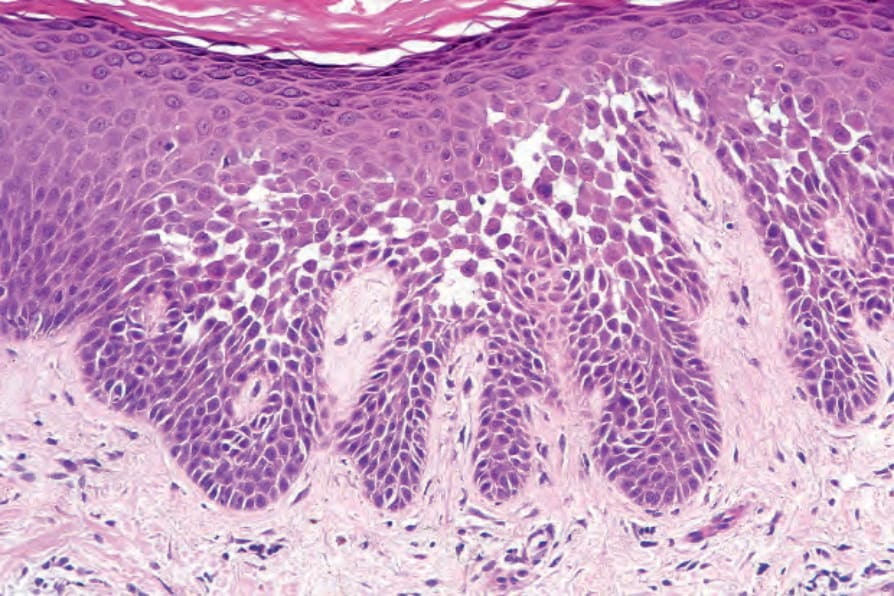
Fig. 5.46 Hailey-Hailey disease: early lesion showing the characteristic ‘dilapidated brick wall’ appearance.
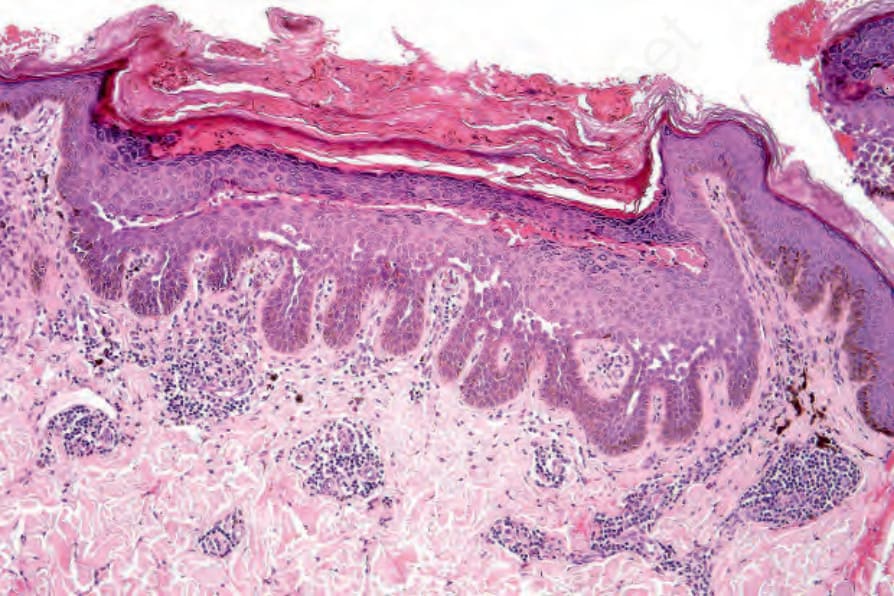
Fig. 5.47 Hailey-Hailey disease: in this example, there is marked hyperkeratosis, parakeratosis, and acanthosis. Villi project into the blister cavity.
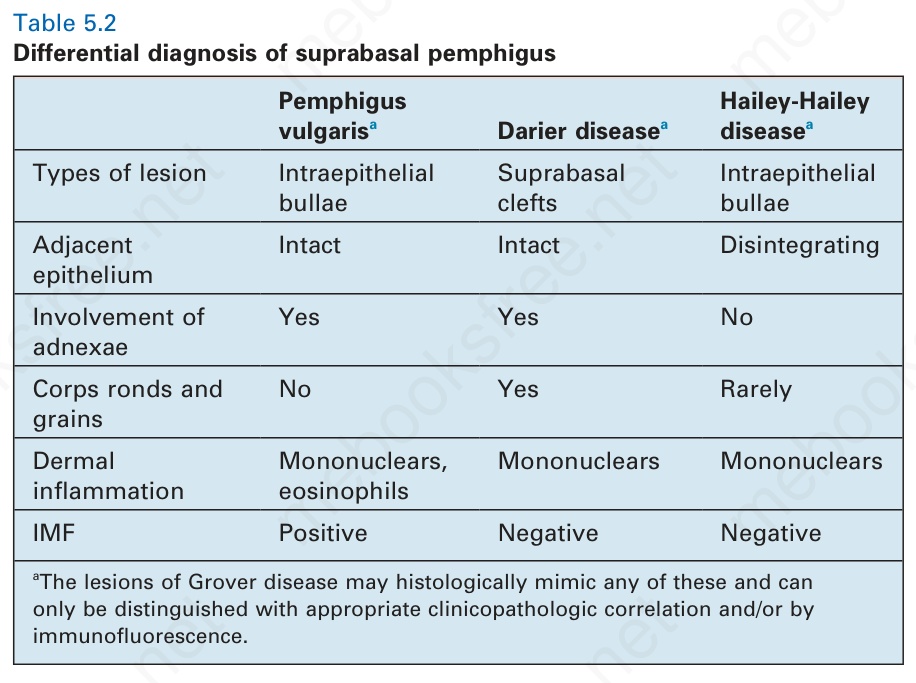
Table 5.2 Differential diagnosis of suprabasal pemphigus