Drug-induced pemphigus
Drug-induced pemphigus
There are at least 25 drugs that have been shown to be associated with the development of pemphigus.1 Penicillamine and captopril are the most common offenders; however, bucillamine, enalapril, cetapril, ramipril, propranolol, bisoprolol, glibenclamide, cilazapril, penicillins, cephalosporins, rifampicin, pyrazolon derivatives, lisinopril, thiopronine, sulfasalazine, and antiseizure medications, among others, have also been implicated.1–11 Some drugs such as penicillamine may elicit either p. foliaceus or p. vulgaris, but the former is much more common.
Symptoms disappear in most patients following withdrawal of causative drugs that contain a sulfhydryl group (thiol drugs). Nonthiol drugs are much less likely to be associated with remission following withdrawal.2
Histologically, in the SPD variant, vesicles are typically found in a subcorneal location associated with a neutrophil infiltrate. It is thought that the presence of IgA is responsible for the striking neutrophil response of this disorder since IgA is associated with neutrophil chemotaxis and neutrophils bear IgA receptors.43,44
In the IEN variant, the pustules can be distributed throughout all layers of the epidermis and may also involve the hair follicles (Figs 5.41 and 5.42).18 Acantholytic cells are usually (but not always) present. Typically, they are sparse and, as such, this diagnostic clue may be very easily overlooked.11–13 Prominent dyskeratotic cells have been described in a rare case of IgG/ IgA pemphigus.45 Significant numbers of eosinophils may also be seen in occasional IEN cases.20,46 Neutrophil dermal papillary microabscesses have also been described, sometimes accompanied by neutrophil spongiosis.12,20 A perivascular infiltrate of neutrophils, lymphocytes, and histiocytes surrounds the superficial vascular plexus, and eosinophils may also sometimes be present. In addition to the major variants characterized by pustules, some patients with IgA pemphigus show histologic features typical of classic p. vulgaris, p. foliaceus, or even, exceptionally, p. vegetans.4,18
Histologically, drug-induced pemphigus resembles sporadic counterparts with positive direct immunofluorescence in most, but not all, patients.12 As expected, given the different variants of pemphigus that drugs may induce, antibodies against both Dsg1 and Dsg3 have been documented.9,13 It has been suggested that a monoclonal antibody against desmogleins 1 and 3 may be useful in the diagnosis and prognosis of drug-induced pemphigus.14 Staining with this antibody is usually patchy in idiopathic pemphigus and diffuse in drug-induced pemphigus. Furthermore, cases of drug-induced pemphigus with diffuse pattern tend to have a poorer prognosis.
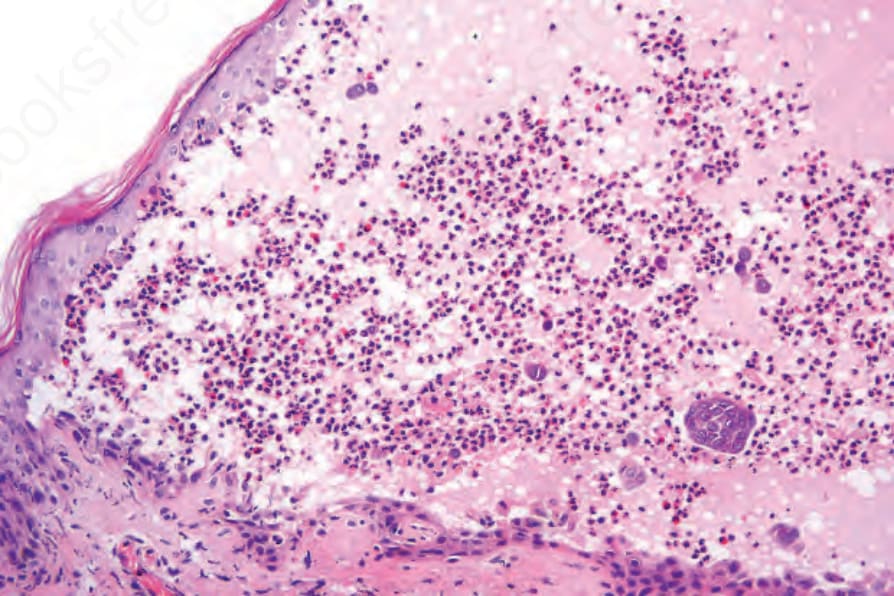
Fig. 5.41 IgA pemphigus: this biopsy is from the edge of an established blister. Note the heavy inflammatory cell infiltrate and focal acantholysis.