IgA pemphigus
IgA pemphigus
Clinical features IgA pemphigus is a rare dapsone-responsive variant of pemphigus that, as its name suggests, is characterized by intercellular IgA deposition and presents clinically with pustular rather than bullous or vesicular lesions.1–6 This disease has been described under a number of different names, such as intraepidermal neutrophilic IgA dermatosis, IgA p. foliaceus, IgA herpetiform pemphigus, intraepidermal IgA pustulosis, intercellular IgA dermatosis, and intercellular IgA vesiculopustular dermatosis.7–16 Most patients are middle-aged or elderly, but children may also be affected.8,17–21 The sex incidence is equal. There is no racial or geographic predilection.8,11 Drug-induced variants have occasionally been documented.22
IgA pemphigus is divided into two major subtypes: subcorneal pustular dermatosis (SPD) variant (IgA p. foliaceus) and intraepidermal neutrophilic IgA dermatosis (IEN) variant (IgA p. vulgaris).7 Other less readily classifiable variants, termed atypical IgA pemphigus, may also be encountered.23
• Patients with SPD-like IgA pemphigus present with superficial flaccid pustular lesions, often arising on an erythematous base and typically affecting the trunk and proximal limbs, although the intertriginous sites are predilected.11 Very uncommonly, there is exclusive involvement of the oral mucosa and perianal skin.24 Occasionally, there is generalized skin involvement. Lesions are crusted and progress with peripheral extension to form ringlike and rosette patterns.15 The features may be indistinguishable from classical non-IgA-associated SPD.
• Patients with the IEN IgA dermatosis variant present with generalized pustules and crusts and erythematous macules with peripheral vesicles forming the so-called sunflower-like configuration (Figs 5.39 and 5.40).7 A dermatitis herpetiformis-like presentation with grouped edematous papules may also be encountered.11,12,15
Pruritus is common and is sometimes severe.8
The lesions in occasional patients resemble classic p. vulgaris or p. foliaceus. In one childhood case, a p. vegetans-like presentation associated with α1-antitrypsin deficiency was documented.18 Mucous membrane involvement in either variant is exceptional.17 Nikolsky sign has been reportedly negative at least in a subset of patients.2,12,13 IgA pemphigus tends to be a chronic relapsing but relatively benign disorder.11,12,15
A significant number of patients (approximately 20%) may have an associated monoclonal gammopathy, usually of the IgA class.11,25–27 Two documented cases have been benign, and the others have represented B cell lymphoma or multiple myeloma.11
Pathogenesis and histologic features SPD IgA pemphigus is characterized by intercellular IgA deposition in the upper epidermis, and circulating IgA antibodies that preferentially bind to the upper epidermis are typically present.4 In contrast, in the IEN variant, IgA is deposited preferentially in the lower epidermis, and circulating antibodies also generally bind to the lower epidermis. In some patients, however, the IgA antibody binds to the entire thickness of the epithelium.
187 Pemphigus
on immunofluorescent studies. Gram stain and a periodic acid-Schiff (PAS) should always be included in the histologic workup to exclude an infective process.
A linear subcorneal distribution has also been documented.9 Complement is not usually present and IgM is absent.7 IgG is typically absent, but there are rare cases of atypical pemphigus with both IgG and IgA that likely represent an unusual form of IgA pemphigus.28,29 The antibodies are of the IgA1 subclass and are usually of low titer.4,17 They have been identified in approximately 50% of patients.12
By immunoelectron microscopy performed on a limited number of cases, the immunoglobulin has been identified within the intercellular space, on the keratinocyte cell membrane, in some cases showing desmosomal accentuation.30–32 In the SPD type, labeling has been predominantly detected in extracellular spaces between keratinocytes at desmosomes, whereas labeling is mainly in intercellular spaces in nondesmosomal areas in the IEN variant.33
The two subtypes result from autoantibody production to different desmosomal proteins.34 Patients with the SPD variant show reactivity with desmocollin 1.35–38 In contrast, anti-Dsg1 or anti-Dsg3 IgA antibodies are present in the IEN variant.19,39–41 One patient with the SPD variant showed both anti-Dsc1 as well as anti-Dsg1 IgA.42 In some patients, however, neither desmocollins nor desmogleins appear to be involved, suggesting that IgA pemphigus is a heterogeneous group of conditions.13,18,38,41

Fig. 5.39 IgA pemphigus: erythematous lesions and an intact vesicle are present. From the slide collection of the late N.P. Smith, MD, the Institute of Dermatology, London, UK.

Fig. 5.40 IgA pemphigus: high-power view showing pus-filled intact blisters and an erosion. From the slide collection of the late N.P. Smith, MD, the Institute of Dermatology, London, UK.
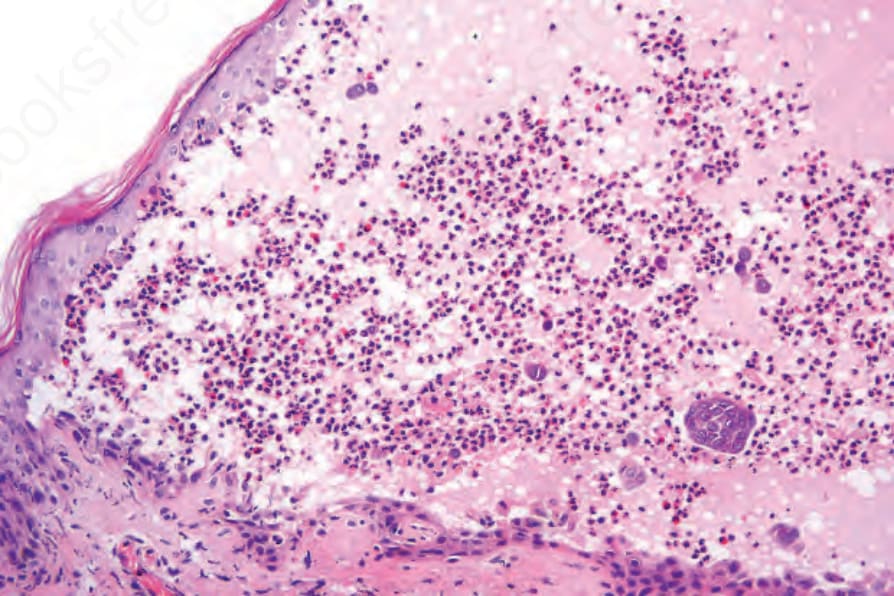
Fig. 5.41 IgA pemphigus: this biopsy is from the edge of an established blister. Note the heavy inflammatory cell infiltrate and focal acantholysis.
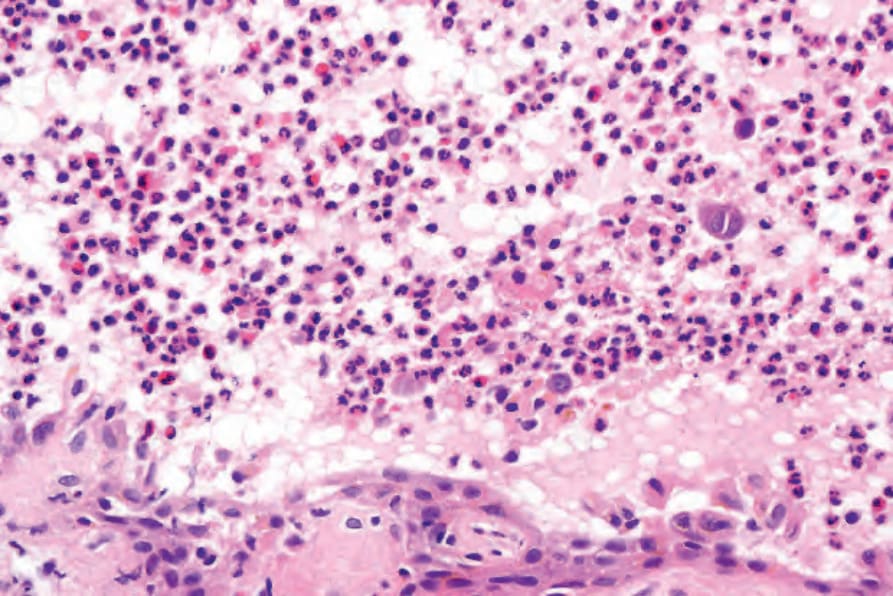
Fig. 5.42 IgA pemphigus: the blister cavity contains neutrophils and eosinophils.