Paraneoplastic pemphigus
Paraneoplastic pemphigus
Clinical features Paraneoplastic pemphigus is a variant of pemphigus, quite distinct from p. vulgaris and p. foliaceus.1 Paraneoplastic pemphigus may be associated with a variety of tumors, such as B-cell lymphoproliferative disorders and hematopoietic malignancies, Castleman disease, Waldenström macroglobulinemia, thymoma (occasionally with myasthenia gravis), Hodgkin lymphoma, carcinomas (e.g., carcinoma of bronchus, pancreas, liver, uterus, breast, thyroid, and liver), and sarcomas (including dendritic follicular cell sarcoma, round cell liposarcoma, leiomyosarcoma, and inflammatory myofibroblastic tumor).2–48 We have seen an exceptional association with systemic mastocytosis. Lymphoma is most often the coexistent neoplasm.1 In a case of a patient with non-Hodgkin lymphoma, the disease developed only after six cycles of fludarabine, raising the possibility of an association with the medication.49 Rarely, patients presented with a disease fulfilling the diagnosis of paraneoplastic pemphigus by histology, immunoblotting, and immunoprecipitation but with no underlying neoplasms have been reported.50–54
• histopathological changes of keratinocyte necrosis, intraepidermal acantholysis, and vacuolar-interface dermatitis,
• direct immunofluorescence showing intercellular IgG and complement accompanied by linear or granular complement at the dermal–epidermal junction (Fig. 5.35),
• indirect immunofluorescence showing circulating antibodies to simple, columnar, and transitional epithelia in addition to a more typical pemphigus pattern of binding to skin and mucosa,
• circulating autoantibodies that immunoprecipitate a high molecular weight complex of polypeptides from keratinocyte extracts weighing 250, 230, 210, 190, and 170 kD. Although the disease may develop in a wide age range (7–83 years), the majority of patients have been in the fifth to eighth decades, and there is a male predominance.5 Exceptionally, children may be affected.4,56–60 Lesions are seen in both the mucosa and the skin. Patients present with refractory, painful, persistent erosions of the oral mucosa and vermilion border of the lips. In addition, the tongue, gingiva, floor of mouth, palate, oropharynx, and nasopharynx can be affected.5 Manifestation confined to the skin or oral mucosa is exceptional.22,61,62 Esophageal disease has been described, and the trachea and bronchi may be affected.63–65 The latter may be accompanied by an invariably fatal bronchiolitis obliterans-like disorder in 6–29% of patients.46,64–69 Colonic involvement is unusual.70 Frequently, patients also have severe pseudomembranous conjunctivitis with symblephara, and
Paraneoplastic pemphigus has been defined by Sapadin and Anhalt as follows55:
• painful mucosal erosions and a polymorphous skin eruption in the context of an occult or confirmed neoplasm (Fig. 5.34),
eventual blindness may occur.5,71 The vulva, vagina, and penis are sometimes affected.4 Myasthenia gravis may be seen in up to 35% of patients with paraneoplastic pemphigus.72 Rarely, the disease is accompanied by alopecia areata.62
Cutaneous lesions are typically polymorphic and often present as a pruritic papulosquamous dermatosis with subsequent blistering. The trunk, proximal extremities, palms, and soles are characteristically affected.73 Nail involvement may occur. Although the eruption typically resembles p. vulgaris, it may also mimic p. foliaceus, IgA pemphigus, bullous pemphigoid, linear IgA disease, lichen planus pemphigoides, erythema multiforme, and toxic epidermal necrolysis.39,74–80 P. vegetans-like lesions have been described.50 Paraneoplastic pemphigus is associated with a very high mortality.5,80
185 Pemphigus
Pathogenesis and histologic features In paraneoplastic pemphigus, circulating antibodies bind to desmosomal and hemidesmosomal plakin family members including 250-kD (desmoplakin I), 230-kD (bullous pemphigoid antigen), 210-kD (desmoplakin II), 210-kD (envoplakin), 190-kD (periplakin), and 170-kD (alpha-2-macroglobulin-like-1, a protease inhibitor) antigens.78,80–84 The presence of antibodies to envoplakin and periplakin (both cornified envelope constituents) is believed to be highly specific for paraneoplastic pemphigus, and the linker domain of plakins may be of particular significance.85,86 Antibodies to Dsg1 and 3 are also usually present and plectin (another plakin family member) antibodies may be found.87,88 Anti-Dsg antibodies are thought to be of particular importance in the initiation of lesions, disrupting the cell membrane and thereby exposing desmosomal and hemidesmosomal plakin proteins with resultant autoantibody formation.81,89
Direct immunofluorescence shows IgG deposition affecting the whole thickness of the epidermis, whereas C3 is found only on the lower layers.80,81,90–92 Characteristically, the intercellular staining is often focal and faint.90,91 In addition, complement C3 is present along the basement membrane region. Immunoglobulin deposition, specifically anti-epiplakin, in the respiratory epithelium has also been documented.63–65,67 Indirect studies confirm the presence of a circulating antibody although the membrane deposition is often masked by strong cytoplasmic labeling.81 This latter can be reduced or abolished by serum dilution.81
In paraneoplastic pemphigus, in addition to binding to stratified squamous epithelium, the antibody labels transitional epithelium, pseudostratified respiratory epithelium, small and large intestinal mucosa, and thyroid epithelium.91 It also reacts with myocardium and skeletal muscle. Rat bladder epithelium is said to be highly specific for paraneoplastic pemphigus.92 Up to 25% of cases, however, are negative.93
Recently, there has been accumulating evidence demonstrating considerable heterogeneity within disorders designated as paraneoplastic pemphigus in addition to overlap with other immunobullous diseases. Patients with additional IgA antibodies against Dsg1, Dsg3, desmocollins, envoplakin, periplakin, bullous pemphigoid antigens, type VII collagen, and laminin 332 have been reported.78,93–97 Immunophenotypic variability among paraneoplastic pemphigus patients has thus been established. The documentation of patients displaying p. vulgaris-like or p. foliaceus-like features has led some authors to suggest that immunobullous disorders arising in association with malignancy would be best viewed as representing a spectrum rather than a distinct entity.74 Included within this spectrum are other nonpemphigus immunobullous disorders resembling erythema multiforme, graft-versushost disease, and lichen planus. The description of antibodies reactive with desmoplakins I and II in some patients with erythema multiforme raises the possibility that these autoantibodies play a pathogenic role in a subset of patients.98 However, further study will be necessary to determine the significance of this finding.
involving adnexal epithelium), and interface changes with basal cell liquefactive degeneration, dyskeratotic keratinocytes, and lymphocytic exocytosis (Figs 5.36–5.38).80,82,101 Spongiosis is often present.3 A perivascular and lichenoid chronic inflammatory cell infiltrate is typically seen in the superficial dermis.85 In some cases, the histologic features may closely simulate lichen planus. A mixture of histological patterns in different biopsies from the same patient is often seen. Eosinophils, however, are rare. Pigmentary incontinence is frequently evident.101
Analogous to other forms of pemphigus, recent studies have suggested a genetic predisposition. HLA typing has identified HLA-Cw14 as the predisposing allele in a Chinese population while DRB103 was identified in a French study.99,100
The histologic findings in paraneoplastic pemphigus are highly variable but are characterized by an admixture of suprabasal acantholysis, often resembling p. vulgaris, with cleft or vesicle formation (sometimes
Acantholysis-like change has also been described affecting the bronchial lining epithelium and brochiolitis obliterans-like features may be seen.63,65
Differential diagnosis The biopsy findings of admixed acantholysis and interface change appear to be relatively non-specific. This contention is demonstrated by skin lesions in patients with typical autoimmune pemphigus without evidence of neoplasia that have histologic features considered typical of paraneoplastic pemphigus.92
The differential diagnosis includes mainly interface dermatitides (e.g., drug eruption, lichen planus, erythema multiforme, graft-versus-host disease)
186 Acantholytic disorders
rather than other variants of pemphigus. A very high index of suspicion on the part of the pathologist and clinician alike and confirmatory immunofluorescence studies are prerequisites to achieving a correct diagnosis.

Fig. 5.34 Paraneoplastic pemphigus: there are numerous erosions and crusted lesions. Courtesy of the Institute of Dermatology, London, UK.
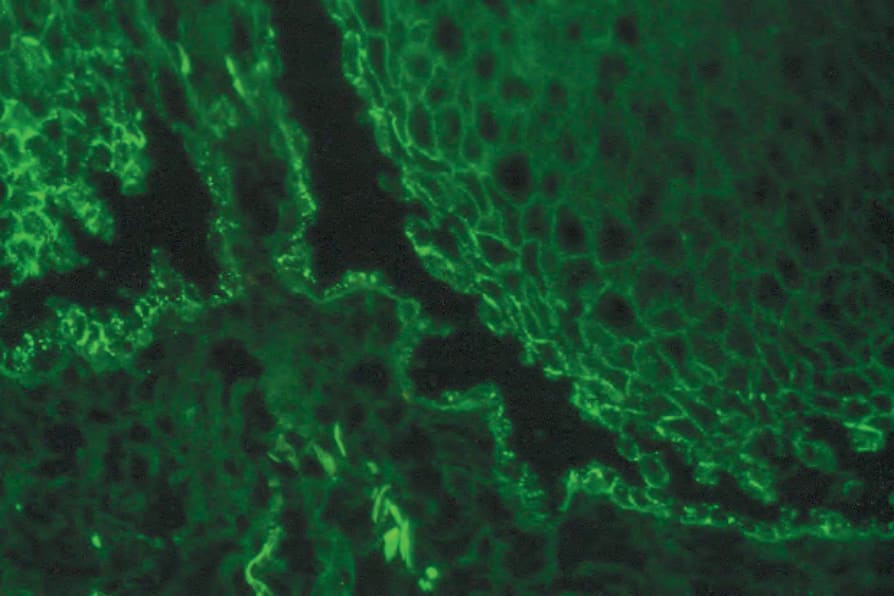
Fig. 5.35 Paraneoplastic pemphigus: IgG is evident in an intercellular distribution.
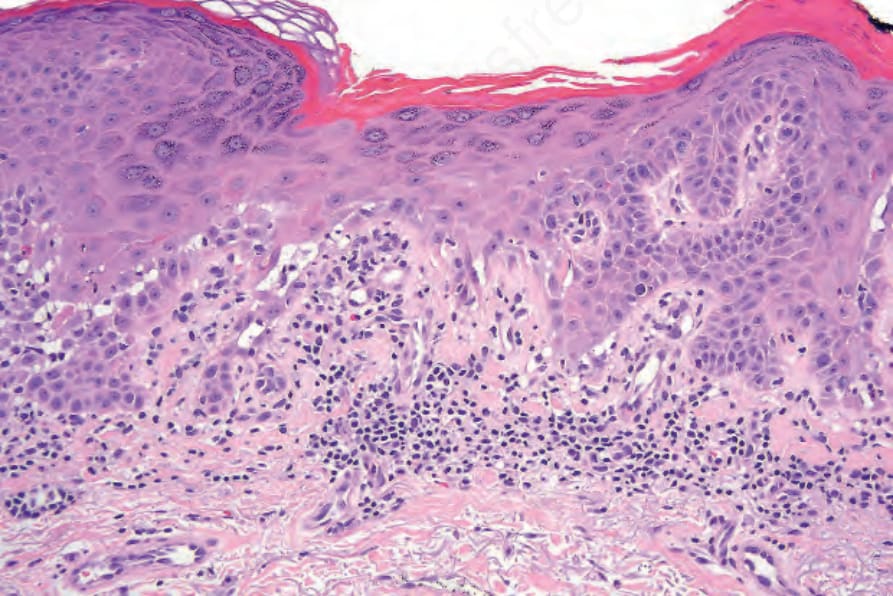
Fig. 5.36 Paraneoplastic pemphigus: this medium-power view shows suprabasal acantholysis and interface change. Note the hyperkeratosis and hypergranulosis. Courtesy of N. Brinster, MD, Virginia Commonwealth University Medical Center, Richmond, Virginia, USA.
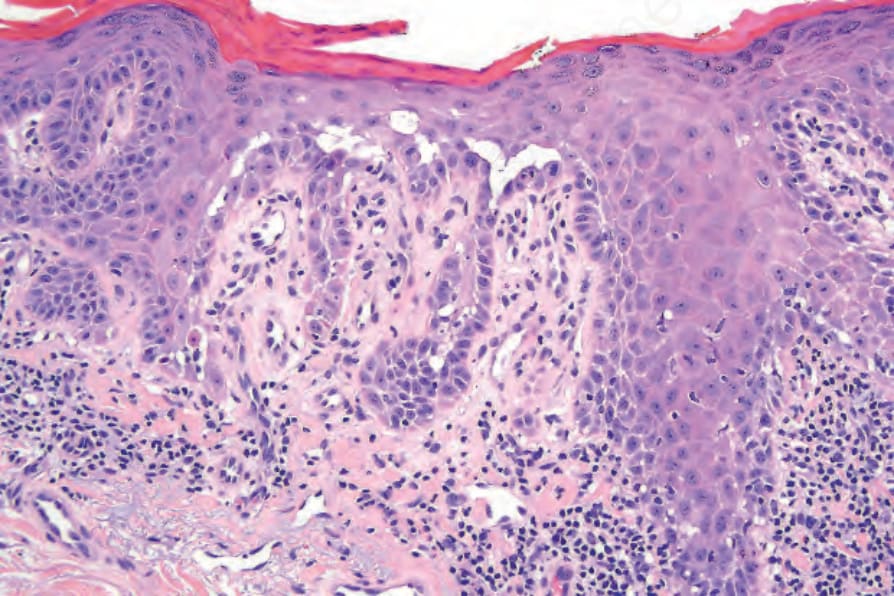
Fig. 5.37 Paraneoplastic pemphigus: higher-power view of acantholysis with suprabasal cleft formation. Courtesy of N. Brinster, MD, Virginia Commonwealth University Medical Center, Richmond, Virginia, USA.
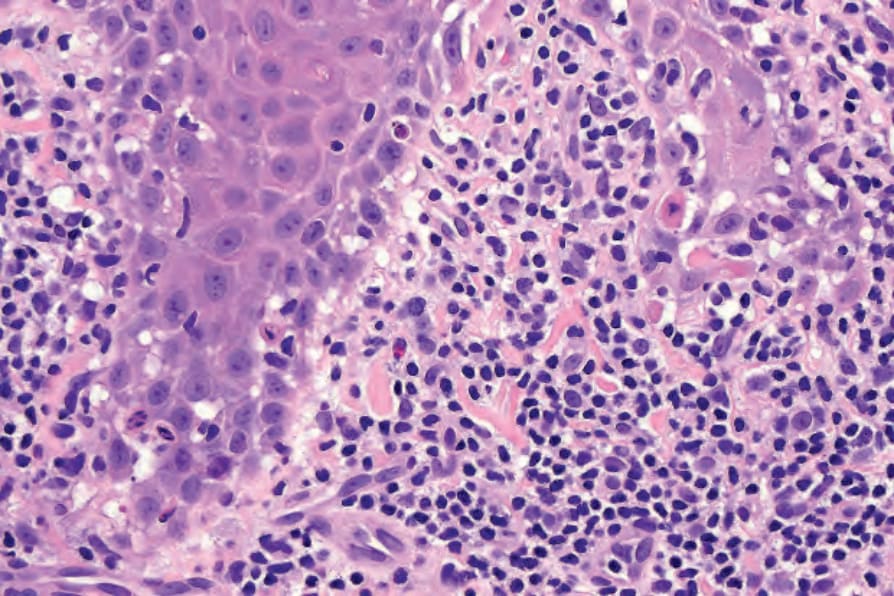
Fig. 5.38 Paraneoplastic pemphigus: note the basal cell hydropic degeneration and cytoid bodies. There is an intense lymphohistiocytic infiltrate. A single eosinophil is evident. Courtesy of N. Brinster, MD, Virginia Commonwealth University Medical Center, Richmond, Virginia, USA.