Pemphigus erythematosus
Pemphigus erythematosus
Clinical features P. erythematosus (Senear-Usher syndrome) is a mild localized form of superficial pemphigus with the histologic and immunofluorescent findings of p. foliaceus combined with features of lupus erythematosus.1–6 In general, the latter is subclinical, being suggested only by laboratory findings, but there are also rare reports of full-blown systemic disease being present.4 The condition shows a worldwide distribution and a slight female predominance.5 Exceptionally, it has been described in children although immunological confirmation of the diagnosis is available in only one case.7–10
Clinically, it is commonly confined to the head, neck, and upper trunk, and typically resembles p. foliaceus. Lesions are erythematous, scaly, and crusted, with or without superficial vesicles, blisters, or erosions. Facial involvement often shows a butterfly distribution reminiscent of lupus erythematosus or seborrheic dermatitis (Fig. 5.31).1 Mucous membrane involvement is exceedingly rare.2
There are reports of p. erythematosus developing after treatment with a number of drugs, notably D-penicillamine, and there are also instances attributed to therapy with propranolol, captopril, pyritinol, thiopronine, ceftazidime, cefuroxime, and atorvastatin.11–16 P. erythematosus has also been described as a complication of heroin abuse.17 In p. foliaceus patients misdiagnosed as having psoriasis, phototherapy can induce p. erythematosus with a positive lupus band test.18
P. erythematosus may rarely be associated with thymoma.3,19–21 Typically, the thymoma precedes the onset of cutaneous lesions, which often present following thymectomy.20,21 Most tumors have been benign, but one
malignant variant has been documented.22 P. erythematosus may also be a manifestation of paraneoplastic pemphigus.3
Pathogenesis and histologic features P. erythematosus, in addition to intercellular staining, also shows granular deposition of IgG and complement along the basement membrane region (positive lupus band test) (Figs 5.32 and 5.33).2,23,24 Typically the latter deposits are found within sun-exposed skin, but in some patients normal, non-sun-exposed skin may also be positive.2 Pemphigus antibody is generally present on indirect immunofluorescence, and antinuclear factor may also be identified.23,24 Anti-DNA antibodies and antibodies to extractable nuclear antigens are negative except in those patients with features of systemic lupus erythematosus.4 In common with p. foliaceus, the antibody
184 Acantholytic disorders
reacts with Dsg1.25 In p. foliaceus patients, circulating anti-Dsg1 precipitate a cleaved off ectodomain of Dsg1 along the basement membrane.18 This may account for the positive lupus band test in p. erythematosus.
P. erythematosus has histologic changes that are identical to those seen in p. foliaceus and fogo selvagem. As the blisters are superficial, it is often very difficult to obtain an intact lesion for diagnosis. Usually, the cleft or blister lies within the granular layer or beneath the stratum corneum. As with the other forms of superficial pemphigus, acantholysis is frequently difficult to detect, but usually a few acantholytic cells can be found attached to the roof or floor of the blister. The blister may contain numerous acute inflammatory cells, particularly neutrophils, which can make distinction from subcorneal pustular disorders especially difficult.
Differential diagnosis The differential diagnosis includes the other forms of superficial pemphigus (p. foliaceus and fogo selvagem), bullous impetigo, and staphylococcal scalded skin syndrome, in addition to subcorneal pustular dermatosis. Distinction depends on a careful consideration of the clinical information, the results of bacterial culture, and immunofluorescence studies.
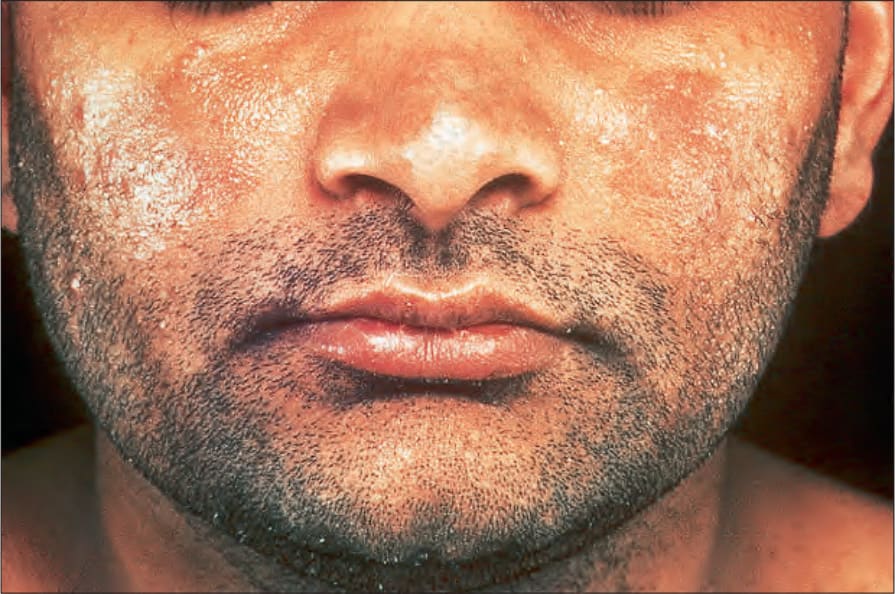
Fig. 5.31 Pemphigus erythematosus: there is scaliness and erythema affecting both cheeks. By courtesy of the Institute of Dermatology, London, UK.
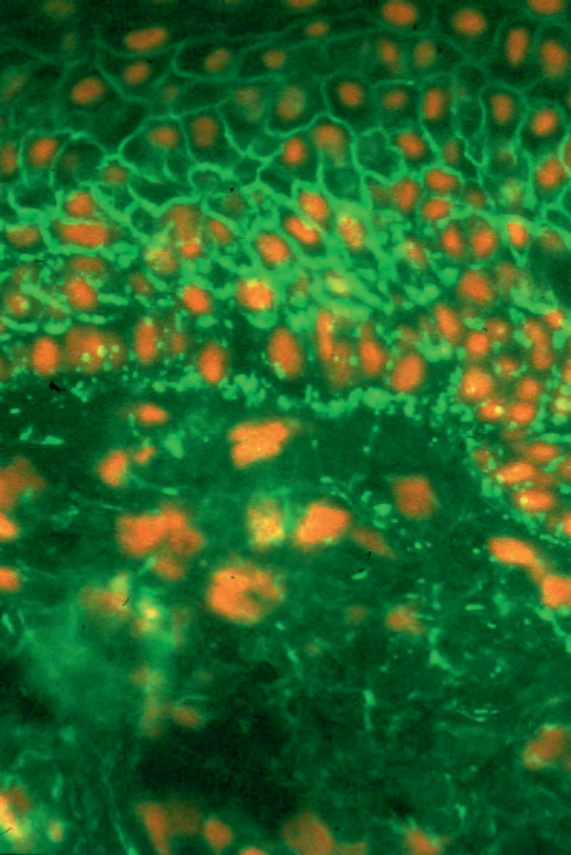
Fig. 5.32 Pemphigus erythematosus: typical intercellular immunofluorescence with granular staining (IgG) at the basement membrane region. By courtesy of B. Bhogal, FIMLS, Institute of Dermatology, London, UK.
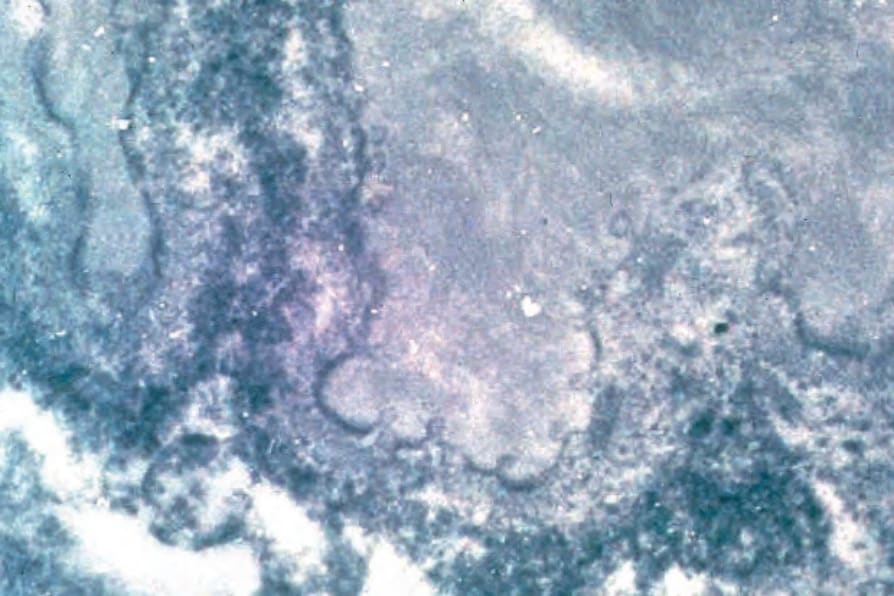
Fig. 5.33 Pemphigus erythematosus: immunoelectron micrograph showing immunoreactant beneath the lamina densa in addition to occupying the intercellular space. By courtesy of B. Bhogal, FIMLS, Institute of Dermatology, London, UK.

Fig. 5.34 Paraneoplastic pemphigus: there are numerous erosions and crusted lesions. Courtesy of the Institute of Dermatology, London, UK.