Endemic pemphigus foliaceus (fogo selvagem)
Endemic pemphigus foliaceus (fogo selvagem)
Clinical features Fogo selvagem (Brazilian p. foliaceus, ‘wild fire’, endemic p. foliaceus) is endemic in regions of Brazil and has also been documented in other areas of Central and South America including Colombia, El Salvador, Paraguay, Venezuela, and Peru.1–12 An endemic area has also been described in Tunisia.13,14 The condition is associated with poverty and malnutrition and particularly affects children and young adults. Results from a more recent epidemiological study demonstrated disease manifestation also in patients of higher socioeconomic class and urban areas.15 There is a striking familial incidence.4 Most cases are found along major rivers, and people especially at risk include farmers and workers involved in land clearing and road construction.2 It appears that the majority of patients live at an altitude of between 500 and 800 meters, and that their homes are generally within 10–15 kilometers of running fresh water and in the path of prevailing winds, thus suggesting an insect vector.4,16 In support of this, a case-controlled epidemiological study has provided evidence that bites by the black fly (family Simuliidae) are a significant risk factor for development of the disease, and it has been proposed that a component of the saliva may trigger an antibody response in susceptible individuals.17–20 Simulium nigrimanum, which is found in the same areas in which Brazilian fogo selvagem occurs, has been identified as being the likely species involved.18
Pathogenesis and histologic features The immunological features of fogo selvagem are similar to p. foliaceus. Indirect immunofluorescent techniques show that the sera of patients with fogo selvagem contain an IgG4 antibody that reacts with Dsg1.16,29 Passive transfer of this antibody to BALB/c neonatal mice results in acantholysis and subcorneal blistering clinically indistinguishable from that of human disease.30–32 Low-titer IgG1 and IgG2 antibodies may also be present, and nonpathogenic IgG1 antibodies are present in unaffected individuals and in the preclinical stages of patients from endemic areas.16,30 IgG antibodies may be accompanied by IgM antibodies, a finding seen more frequently in individuals from rural rather than urban areas. IgM and IgE antibodies are detected more frequently associated with fogo selvagem than p. foliaceus.33,34 Fogo selvagem is otherwise histologically and by immunofluorescence indistinguishable from nonendemic foliaceus and, like the latter, the antibody recognizes epitopes in the ectodomain of Dsg1.35,36 Epitope recognition is conformation specific and calcium dependent, and recently intramolecular epitope spreading has been implicated in the pathogenesis of the disease. Epitope spreading appears to be related to onset of disease as well as disease modulation with remission and relapse.37 Specifically, it has been shown that sera from patients in the preclinical stage or in remission recognize epitopes in the COOH-terminal region of the ectodomain of Dsg1, whereas antibodies against epitopes in the NH2-terminal region of the ectodomain are detected at disease onset.16,37 Interestingly, a study has suggested that the presence of serum IgG4 antidesmoglein-1 in asymptomatic individuals may suggest preclinical disease.38,39 A subset of patients may
The clinical presentation of fogo selvagem has been divided into a number of categories including localized and generalized forms2,4:
• Localized disease presents in a variety of ways including small blisters and erosions or violaceous papules and plaques distributed mainly in the seborrheic areas. Such lesions may be clinically misdiagnosed as discoid lupus erythematosus.
182 Acantholytic disorders
also have antibodies to Dsg3, ranging from < 10% to 36%.40–42 Antibodies to Dsg3 are especially common in the Terena reservation of Liao Verde, Brazil, where additional anti-Dsg3 antibodies were detected.42 Patients have circulating CD4+ memory T cells with a Th2 cytokine profile that proliferate in response to the extracellular domain of Dsg1 and are thought to be of importance in the initiation and progression of the disease by stimulating B cell production of autoantibodies.43–45 The systemic kinin system appears to be activated in patients with fogo selvagem, but the significance of this finding and its mechanism of action in blister formation are unclear.46 The discussion of pathogenesis of the nonendemic form discussed above also apply to the endemic form.
Patients often share the HLA phenotype DRB10102 and lack DQB10201, which is thought to represent a dominant protective gene found in unaffected persons living in endemic regions.38,39 HLA-DRB1*0404, *1402,*1406, or *0102 may also confer susceptibility.4,40,47,48
and periplakin.12,51 Antibodies to pilosebaceous units and surrounding neurovascular structures have also been identified in these patients.52
Recently, criteria have been proposed to establish a diagnosis of fogo selvagem as distinct from nonendemic p. foliaceus4:
• clinical evaluation,
• presence of subcorneal acantholysis,
• positive direct and indirect immunofluorescence and/or immunoprecipitation or ELISA assays,
• confirmatory epidemiological data.
Differential diagnosis As with p. foliaceus, the histologic features in fogo selvagem may be easily overlooked, and a high index of suspicion is critical to making the diagnosis. The differential diagnosis includes p. foliaceus, p. erythematosus, bullous impetigo, staphylococcal scalded skin syndrome, subcorneal pustular dermatosis, and, in some cases, psoriasis. Careful clinical correlation, immunofluorescence studies, and sometimes bacterial culture are necessary to establish a definitive diagnosis.
The histologic changes of fogo selvagem are identical to the other forms of superficial pemphigus (p. foliaceus and p. erythematosus).49 Since the blisters are superficial, often only nonbullous erosions are present for histologic examination. It is very difficult to obtain an intact lesion for diagnosis. Typically, the cleft or blister lies within the upper epidermis, granular layer, or beneath the stratum corneum. Acantholysis is frequently subtle, but usually a few acantholytic cells can be found attached to the floor of the blister. The blister roof is often missing. Blisters may contain numerous inflammatory cells, particularly neutrophils. This feature may cause confusion with infection or other subcorneal pustular disorders. Eosinophilic spongiosis in association with perivascular eosinophils is also sometimes present, particularly if biopsies of early lesions are examined (Figs 5.29 and 5.30).
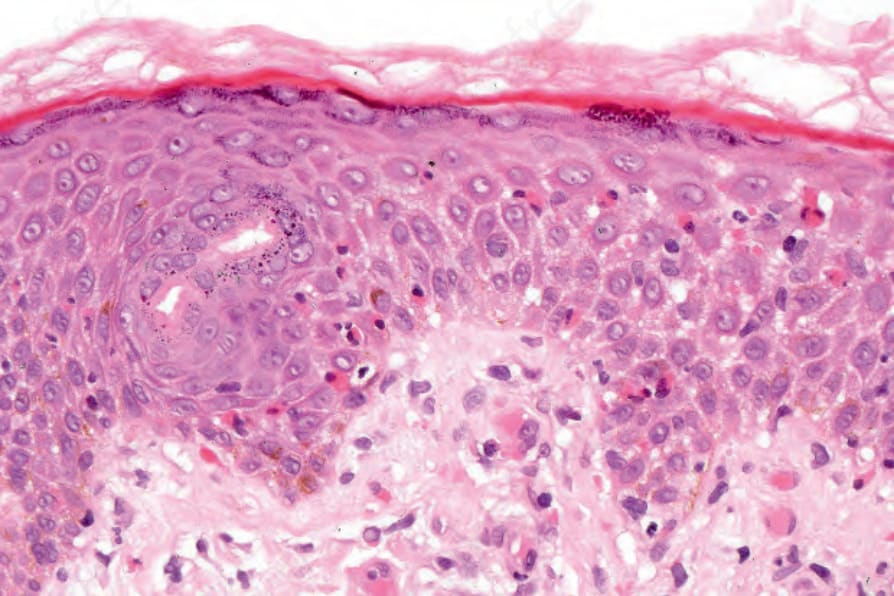
Fig. 5.29 Brazilian pemphigus foliaceus: in this example of an early lesion, the features of eosinophilic spongiosis are evident.
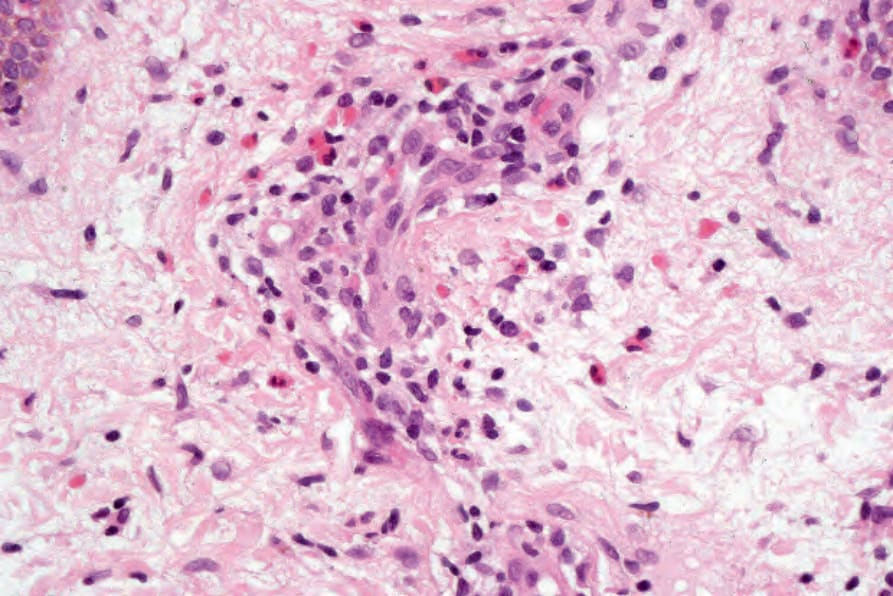
Fig. 5.30 Brazilian pemphigus foliaceus: there is superficial dermal edema and a perivascular inflammatory cell infiltrate with conspicuous eosinophils.