Pemphigus foliaceus
Pemphigus foliaceus
Clinical features P. foliaceus is considerably more uncommon than p. vulgaris, and although it most often affects the middle-aged and elderly, it has a very variable age of onset, sometimes affecting younger adults and even, occasionally, children.1–8 Very exceptionally, maternal antibodies have been known to cross the placenta, resulting in neonatal disease.9–13 In general, nonendemic p. foliaceus in children is relatively benign and of short duration.6
The superficial blisters of p. foliaceus are exceedingly fragile and therefore much less obvious; erosions and large leafy scales or crusts are often predominant (Figs 5.20–5.22). The lesions may remain localized to the scalp, nose, face, and trunk for many months or years, leading to a mistaken diagnosis of seborrheic dermatitis, seborrheic keratosis, or even lupus erythematosus. Sometimes the eruption involves the entire surface of the body or produces a clinical resemblance to exfoliative dermatitis (erythroderma) (Fig. 5.23).14,15 Mucous membrane involvement is rare due to the lack of Dsg1 in oral mucosa (see below).1,16 Exceptionally, patients may
present with localized disease, typically restricted to the face.17,18 The development of pustular lesions is exceptional.19 P. foliaceus often has a much more benign course than p. vulgaris, although patients with severe disease, requiring corticosteroid and immunosuppressant therapy, still have a risk of mortality. The disease may be complicated by Kaposi varicelliform eruption,
179 Pemphigus
A
A
B
B
a disseminated eruption caused by a viral infection (e.g., herpes simplex virus) superimposed on a pre-existing dermatosis.20
Very occasionally, patients may develop p. foliaceus during or after a previous episode of p. vulgaris and vice versa.21–23 The development of bullous pemphigoid following an episode of p. foliaceus has also been described.24,25 This is accompanied by an antigen shift, possibly as a result of intermolecular epitope spreading.22,26–28 A case of a blistering disorder displaying features of bullous pemphigoid and p. foliaceus has been described in association with consumption of Spirulina algae.29 The coexistence of both p. vulgaris and p. foliaceus in the same patient has also been reported.30 A further case of paraneoplastic pemphigus with concomitant clinical features of p. foliaceus and the presence of antibodies against desmoglein 1 has been reported.31
In addition to idiopathic p. foliaceus, drug-induced variants, notably due to penicillamine, may also be encountered (Fig. 5.24). A localized form may also be associated with topical drugs such as imiquimod and has been reported following radiation therapy.32–35 Recently, p. foliaceus related to an anti-TNF-α inhibitor has been reported.36 P. foliaceus is rarely associated with an underlying malignancy including non-Hodgkin lymphoma and esophageal cancer.37,38 An unusual case of p. foliaceus associated with myasthenia gravis and lupus erythematosus has been reported in a patient who underwent a thymectomy for a thymoma.39
Pathogenesis and histologic features Similar to other variants of pemphigus, p. foliaceus is an immunologically mediated disease. Examination of perilesional skin by direct immunofluorescent techniques reveals in vivo-bound immunoglobulin (usually IgG) and
180 Acantholytic disorders
often complement (C3) in the intercellular region of the epidermis.1 Abundant antigen in the follicular outer root sheath and germinal matrix may account for the marked scalp involvement typical of pemphigus.39
Indirect immunofluorescent techniques show that the sera of patients with p. foliaceus contain an IgG antibody that reacts with the intercellular region of normal squamous epithelium.40 IgG4 predominates followed by IgG1.41,42 IgG3 is also sometimes present. This may be of importance since IgG3 is the most efficient activator of complement.41 Some 60–70% of patients have positive indirect immunofluorescence.43
The p. foliaceus antibody binds to a 160-kD desmosomal cadherin, designated Dsg1.44,45 The sera of p. foliaceus patients bind to the extracellular amino terminal domain of bovine Dsg1, whereas sera from both p. vulgaris and p. vegetans patients react with the intracellular domain of Dsg1.46,47 Compared with p. vulgaris, immunofluorescence studies on the sera of p. foliaceus tend to show more staining in the superficial epidermis, correlating with the level of the split.48,49 Conversely, the sera from patients with p. vulgaris show more affinity for the lower epidermis. Anti-Dsg1 antibody is pathogenic.50 Injection of purified anti-Dsg1 antibodies from sera of patients with p. foliaceus into neonatal mice induces subcorneal acantholysis in a pattern typical of p. foliaceus.51 Acantholysis is thought to be the result of an antibody-mediated cellular response rather than purely the result of steric hindrance.52,53 Internalization of nonclustered Dsg1 has been put forward as a possible mechanism resulting in lack of newly formed desmosomes rather than a disruption of pre-existing structures.48,54 Increasing evidence suggests that the blistering is the result of the activation of p38 mitogen-activated protein kinase-dependent signaling by the p. foliaceus IgG antibodies.55 Rarely, patient sera contain additional IgG antibodies directed against Dsg3 and the presence of additional IgA antibodies against Dsg1 as well as Dsg3 has also been detected.3,56,57 Antibodies to desmocollins may also play a role, and at least one case of childhood p. foliaceus secondary to autoantibodies exclusively directed against desmocollins has been described.58 Patients with clinical and histologic features of p. foliaceus but direct immunofluorescence findings reminiscent of p. erythematosus have been reported. Antibodies recognizing bullous pemphigoid antigen 1 (BP230) as well as a 190-kD protein co-migrating with periplakin were detected in these patients in addition to anti-Dsg1 antibodies.59 The use of D-penicillamine may be associated with the acquisition of a pemphigus-like antibody and the development of p. foliaceus.60
A
B
Since the blisters of p. foliaceus are superficial, they are therefore fragile, and it is often very difficult to obtain an intact lesion for diagnosis. Patients commonly have erosions without blisters, and frequently the clinician does not suspect a bullous disorder. Usually, the cleft or blister lies within the upper epidermis (Fig. 5.25) but may also occur in the granular layer or throughout the epidermis.61 The roof of the fragile blister is often not present, having sloughed either before or after biopsy. Acantholysis is frequently difficult to detect, but usually a few acantholytic cells can be found attached to the roof or floor of the blister. In cases where the blister is missing, a careful inspection of the hair follicles may reveal focal acantholysis. In some cases, the acantholysis is subtle, and the biopsy may show features reminiscent of a spongiotic dermatitis (Fig. 5.26). Sometimes the blister contains numerous acute inflammatory cells (Fig. 5.27), particularly neutrophils, which can make distinction from subcorneal pustular disorders, including bullous impetigo, a dermatophyte infection, candidiasis, pustular psoriasis, and subcorneal pustular dermatosis especially difficult.62,63 Eosinophilic spongiosis may also be seen.64 A form with histologic and clinical overlap with psoriasis has also been described.65
Differential diagnosis The histologic features in the superficial forms of pemphigus may be easily overlooked and, since bullae are often not appreciated by the clinician, the unwary pathologist may not consider a bullous disorder when evaluating the biopsy. A high index of suspicion is therefore critical. The differential diagnosis of superficial pemphigus includes bullous impetigo, staphylococcal scalded skin syndrome, IgA pemphigus, subcorneal pustular dermatosis, and psoriasis (Table 5.3). Distinction depends on a careful consideration of the clinical information, the results of bacterial culture, and immunofluorescent studies.
181 Pemphigus
Superficial pemphigus IgA pemphigus Subcorneal pustular dermatosis Pustular psoriasis Reactive arthritis Pustular drug reaction Bullous impetigo Staphylococcal scalded skin syndrome Pustular fungal infection
• Generalized presentation includes bullous exfoliative, exfoliative erythrodermic, and disseminated plaque and nodular (resembling nodular prurigo) variants (Fig. 5.28).4
With resolution, patients may sometimes develop hyperpigmentation.21 Rare cases of neonatal p. foliaceus have been reported, but in most patients the antibody does not cross the placental barrier.22–24 Patients with fogo selvagem appear to rarely have other concomitant autoimmune disorders.24–27
In contrast to Brazilian fogo selvagem, endemic disease in the area of El Bagre, Colombia, shows several unusual and distinguishing features.12,28 The disease affects an older population with a strong male predilection and clinical features reminiscent of p. erythematosus. In addition to the more classical presentation, patients develop hyperkeratotic plaques on the face, chest, and back reminiscent of discoid lupus erythematosus as well as an erythematous macular lesion in a butterfly-like distribution in the central face.12,28 Active disease is also accompanied by conjunctivitis. The disease also shows characteristic immunological and histologic changes, which are discussed below.

Fig. 5.20 Pemphigus foliaceus: multiple erosions are present with background erythema and postinflammatory hyperpigmentation. Courtesy of the Institute of Dermatology, London, UK.

Fig. 5.21 Pemphigus foliaceus: crusted lesions are evident on the back of this young male. From the collection of the late N.P. Smith, MD, the Institute of Dermatology, London, UK.
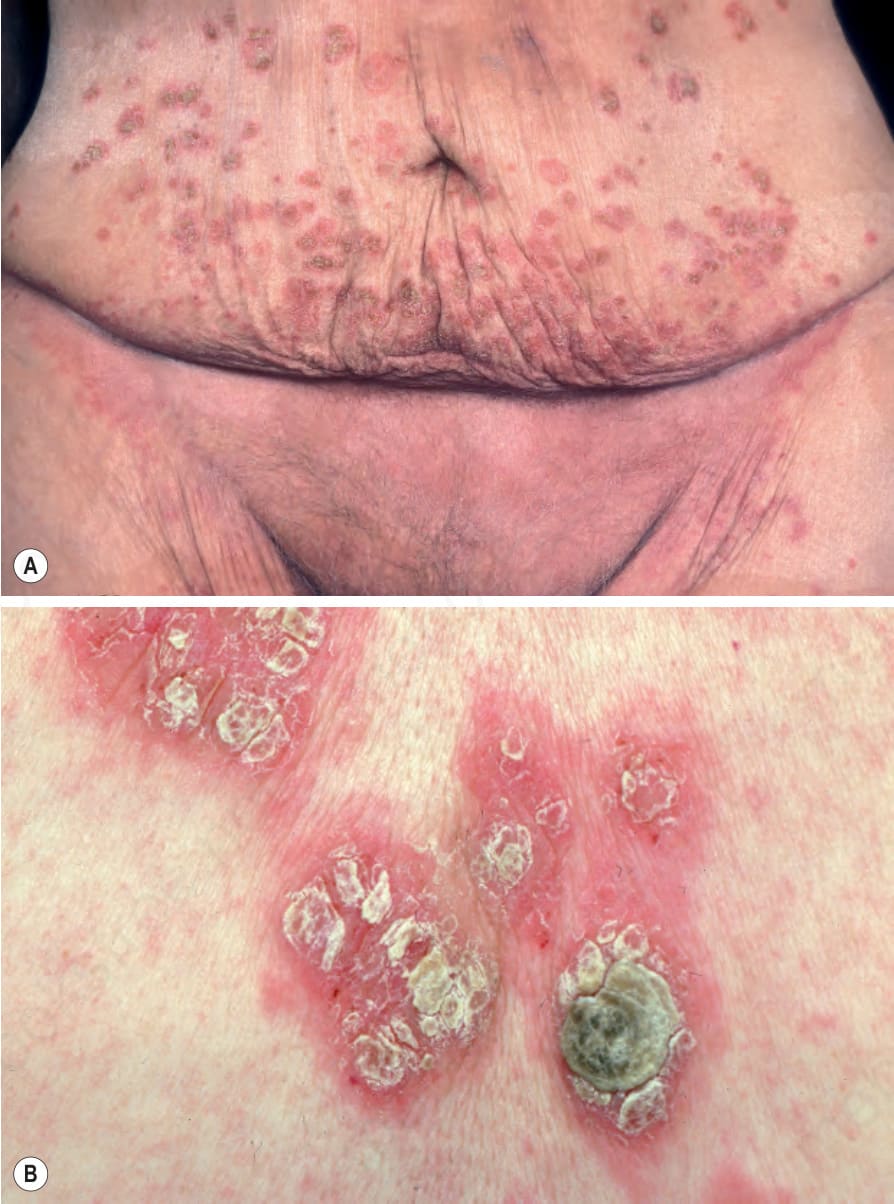
Fig. 5.22 Pemphigus foliaceus: (A) there are numerous crusted lesions on the lower abdomen and in the groin; (B) high-power view. From the slide collection of the late N.P. Smith, MD, the Institute of Dermatology, London, UK.

Fig. 5.23 Pemphigus foliaceus: in this patient, there is generalized erosion with scaling and erythroderma. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.
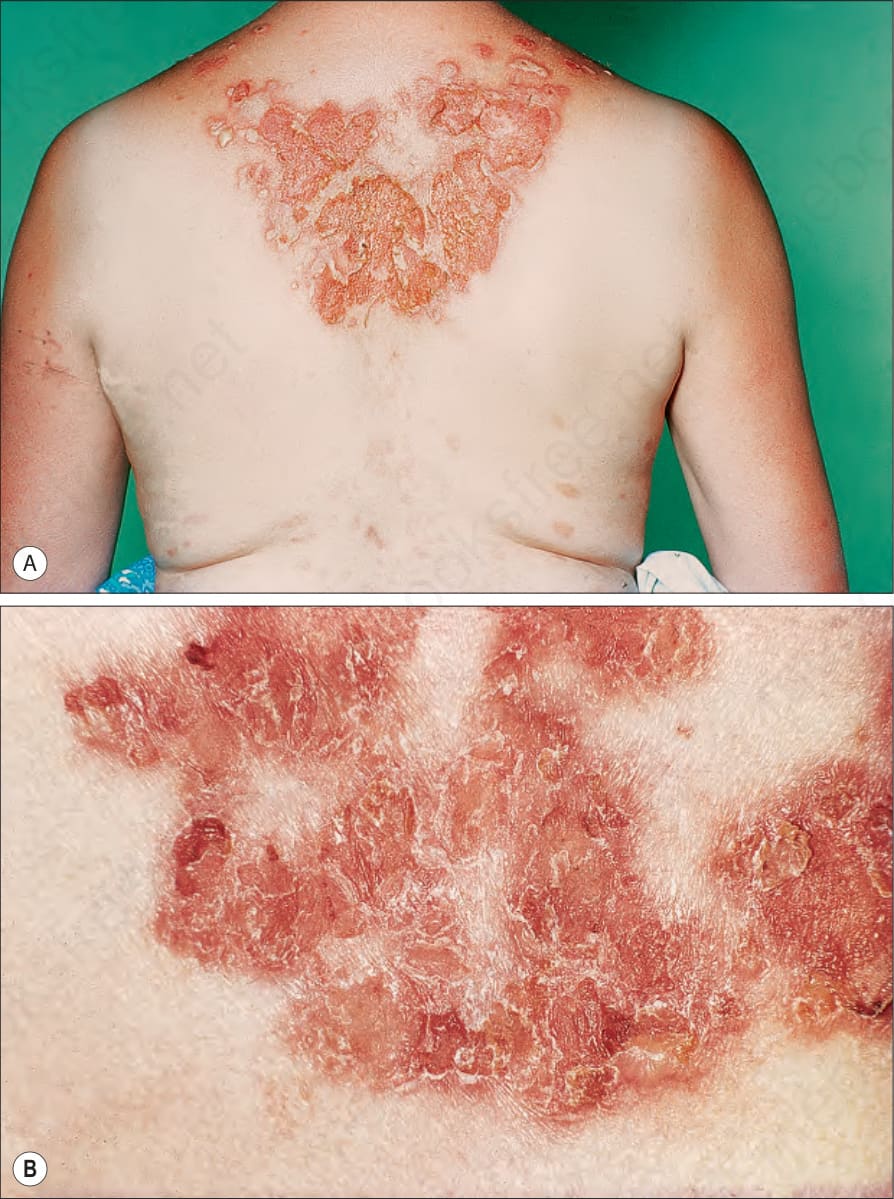
Fig. 5.24 Pemphigus foliaceus: (A) in this patient, the eruption was induced by penicillamine therapy; (B) close-up view of intact blisters, erosions, and crusting. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.
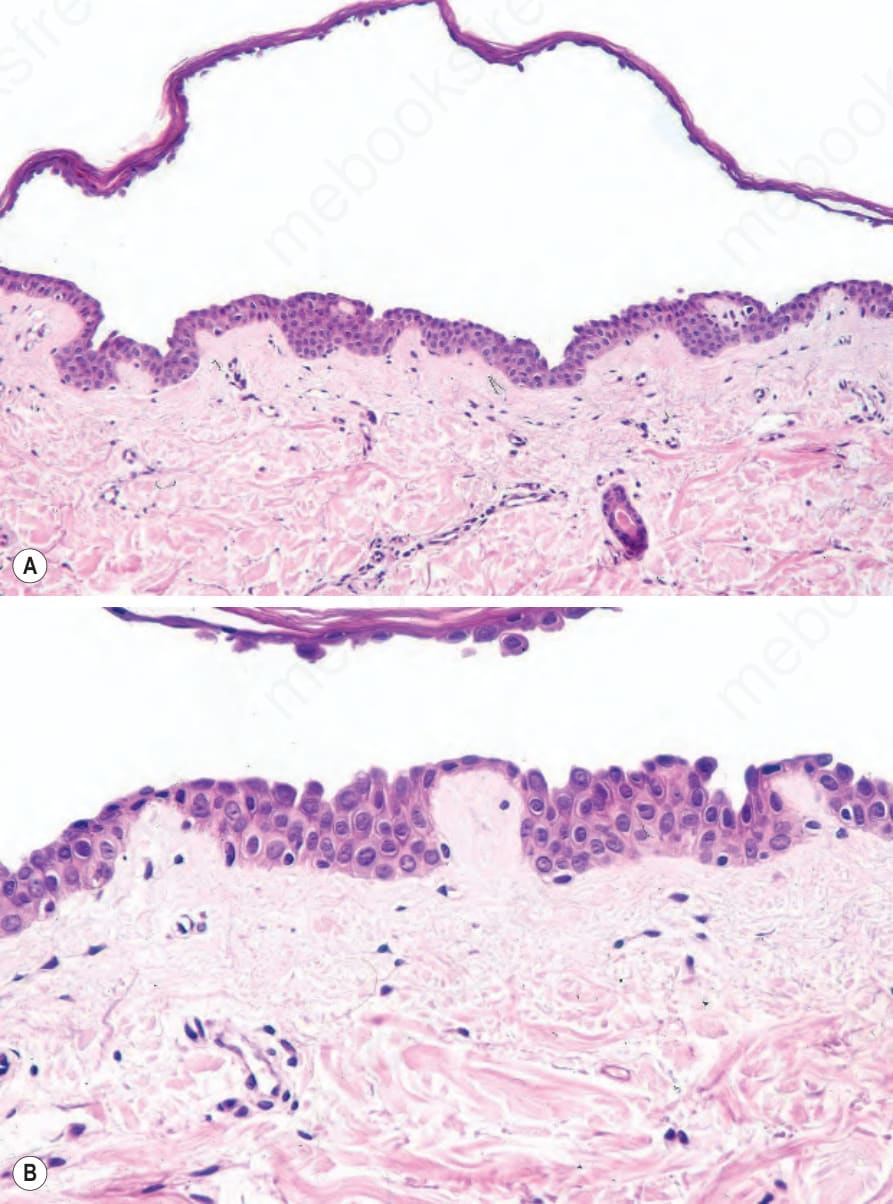
Fig. 5.25 Pemphigus foliaceus: (A) in this example, there is a cell-free, subcorneal blister; (B) occasional acantholytic cells are present adjacent to the roof.
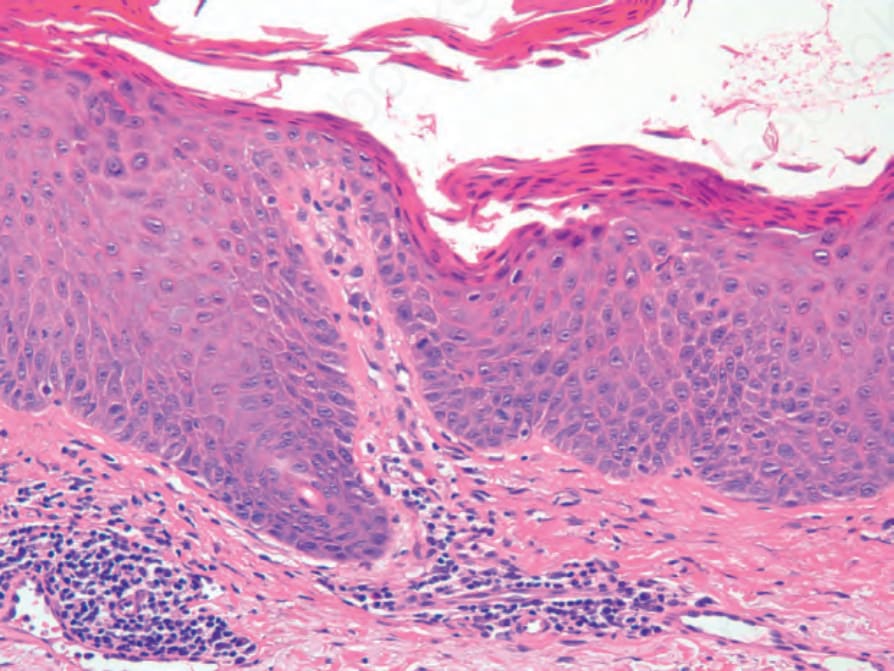
Fig. 5.26 Pemphigus foliaceus: in this example, there is spongiosis resembling a spongiotic dermatitis and only subtle, focal acantholysis.
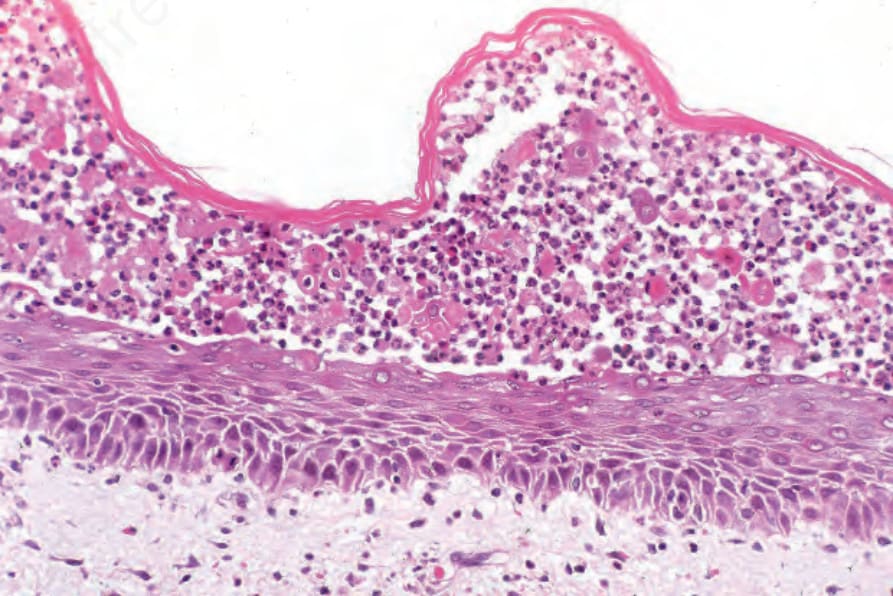
Fig. 5.27 Pemphigus foliaceus: in this example, the blister cavity contains numerous neutrophils. Acantholytic cells are conspicuous.

Fig. 5.28 Brazilian pemphigus foliaceus: this woman with chronic disease shows very severe scaling. Blisters are not apparent. By courtesy of S.A. Pecher, MD, Amazonas, Brazil.
Table 5.3 Differential diagnosis of superficial pemphigus: conditions characterized by subcorneal pustules