Pemphigus vegetans
Pemphigus vegetans
Clinical features P. vegetans, a chronic variant of p. vulgaris, has a somewhat better prognosis than p. vulgaris with occasional cases associated with spontaneous remission documented.1–3 It accounts for 1–9% of all cases of pemphigus and appears to be especially common in North Africa.1,4 As with the vulgaris variant, p. vegetans typically presents in adults. There has, however, been a small number of cases described in childhood including a dapsone-responsive IgA-mediated variant.5–8 The lesions, which present as blisters and erosions, are particularly prolific in the flexures, especially the axillae, the groin, the inframammary region, the umbilicus, and at the margins of the lips. The
Types of lesion Intraepithelial bullae
Suprabasal clefts
Intraepithelial bullae
Adjacent epithelium
Intact Intact Disintegrating
Involvement of adnexae
Yes Yes No
Corps ronds and grains
No Yes Rarely
Dermal inflammation
Mononuclears, eosinophils
Mononuclears Mononuclears
IMF Positive Negative Negative
aThe lesions of Grover disease may histologically mimic any of these and can only be distinguished with appropriate clinicopathologic correlation and/or by immunofluorescence.
177 Pemphigus
scalp is also said to be a site of predilection.9,10 Soon thereafter, patients characteristically develop hypertrophic vegetations and pustules at the blistered edges (Fig. 5.16).1
The oral cavity is commonly affected, and a cerebriform or ‘scrotal’ tongue is said to be a diagnostic clue in cases of early involvement.11–14 An exceptional case of the disease restricted to the tongue has been reported.15 Esophageal involvement presenting as erosions and white plaques has been described in a number of patients, and the nasal mucosa, larynx, vulva, vagina, penis, and anus may also be affected.8,16–20 Nail involvement including onycholysis and pustules is sometimes seen.21 Acral involvement can clinically be mistaken for acrodermatitis continua suppurativa.22 Peripheral blood eosinophilia is commonly present.
Two clinical subtypes are recognized:23,24
• In the Neumann variant (the more serious form), lesions usually begin as described in p. vulgaris, but the ensuing erosions develop vegetations. The course of this variant is similar to that of p. vulgaris.
• In the Hallopeau variant (‘pyodermite vegetante’), the eruption begins as pustular lesions that rapidly evolve into verrucous vegetating plaques.2 Bullae are usually not seen. This is a milder variant in which spontaneous remission is not uncommon.
Pathogenesis and histologic features Support for the thesis that p. vegetans is a variant of p. vulgaris is based on the finding that both subtypes are associated with IgG and C3 deposition in the epidermal intercellular space on direct immunofluorescence, and circulating ‘pemphigus’ antibody.24 P. vegetans is characterized by an antibody directed at the Dsg3.25–27 Antibodies against desmocollins 1 and 2 as well as periplakin have also been documented.28,29 Rarely, additional IgA antibodies to Dsg3 may also be detected.30
Precipitating factors for this pemphigus variant are largely unknown. A case has been described developing after and restricted to a split-thickness skin graft.31 Exceptionally p. vegetans has been linked with the ACE inhibitors captopril and enalapril.32,33 Further exceptional cases developed in association with intranasal heroin or cocaine abuse and HIV infection.20,34–36 There are rare reports relating a p. vegetans-like lesion as a manifestation of paraneoplastic pemphigus and p. vegetans with underlying malignancy.37–42
Although a variant of p. vulgaris, p. vegetans shows strikingly different histologic features. Suprabasal acantholysis is present but is often subtle, being masked by an exuberant proliferation of squamous epithelium, which may sometimes show pseudoepitheliomatous hyperplasia (Fig. 5.17). The epithelial proliferation involves both the epidermis and the infundibular follicular epithelium. Characteristically, there is an intense inflammatory cell infiltrate containing numerous eosinophils, and intraepidermal microabscesses are often seen (Figs 5.18 and 5.19). Eosinophilic spongiosis is often a prominent feature.43,44 The inflammatory changes and epithelial proliferation are sometimes so marked that the true nature of the lesions is obscured. Very occasionally, 10–40-µm eosinophilic hexagonal Charcot-Leyden crystals have been described within the eosinophil-rich microabscesses.32,45 The diagnosis of p. vegetans is easily overlooked and is made only by the pathologist with a high index of suspicion.
178 Acantholytic disorders
Differential diagnosis Given the histologic overlap with p. vulgaris, the same differential diagnosis as discussed for that variant should be considered. In established lesions associated with squamous epithelial hyperplasia, the suprabasal cleft formation is often focal and easily overlooked. Infections, particularly fungal and bacterial, that are associated with pseudoepitheliomatous hyperplasia and microabscesses may be confused with p. vegetans. In particular, pyostomatitis/pyodermatitis vegetans must be excluded in patients presenting with oral involvement. The latter is usually associated with inflammatory bowel disease, and although it may mimic p. vegetans clinically and histologically (acantholysis tends to be focal and is often absent in pyostomatitis), direct immunofluorescence is usually negative. In rare cases however, in pyostomatitis/pyodermitis vegetans direct immunofluorescence may be positive for IgA in the superficial epidermis and/or for IgG and C3 at the dermoepidermal junction. In exceptional cases there seems to be overlap between these conditions and pemphigus.46,47 Halogenoderma (iododerma and bromoderma) may also show similar histological features with prominent eosinophilic spongiosis but in the latter acantholysis is not a feature.

Fig. 5.16 Pemphigus vegetans: axillary ulceration and vegetative lesions. From the slide collection of the late N.P. Smith, MD, the Institute of Dermatology, London, UK.
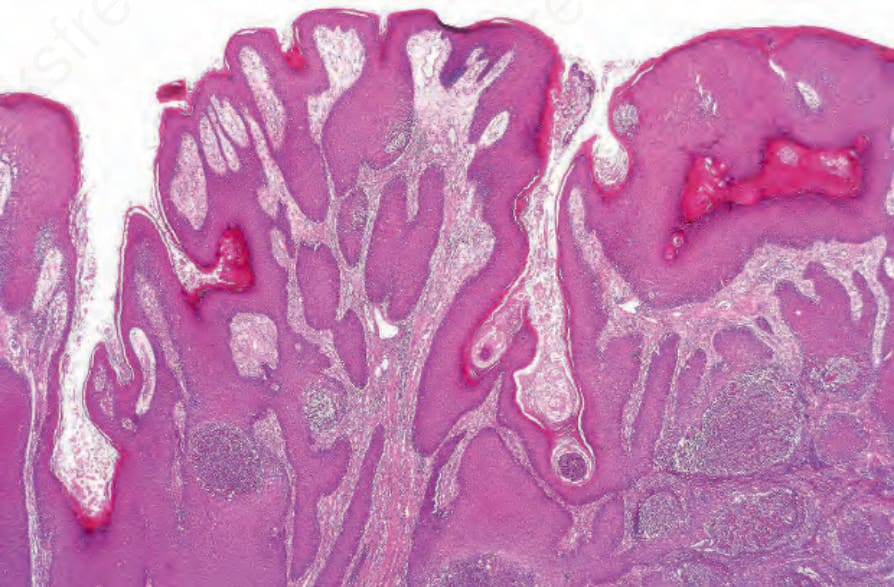
Fig. 5.17 Pemphigus vegetans: the epidermis is hyperplasic and there are scattered abscesses.
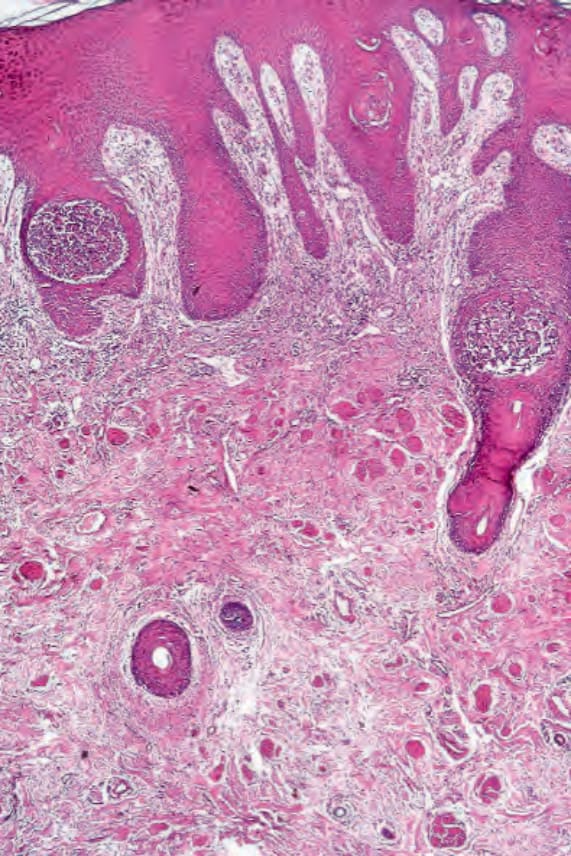
Fig. 5.18 Pemphigus vegetans: follicular involvement is seen on the right.
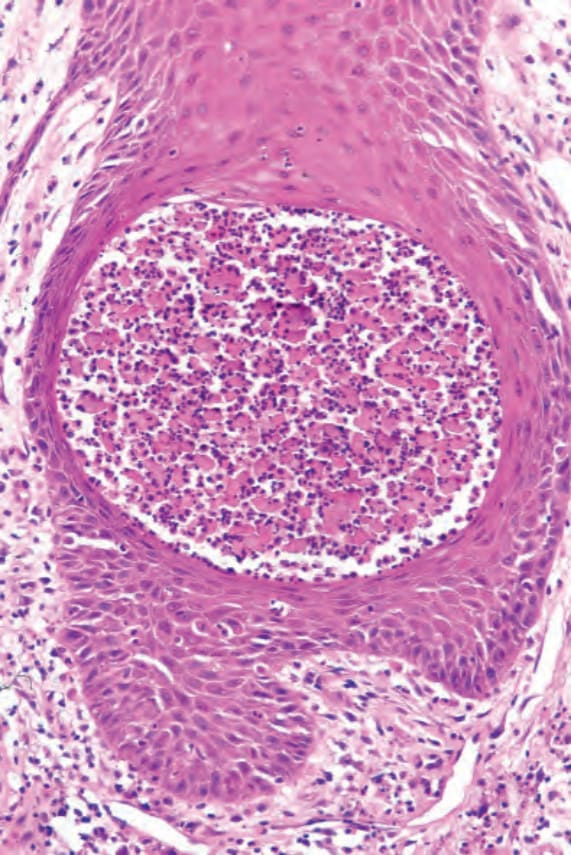
Fig. 5.19 Pemphigus vegetans: there are numerous eosinophils. Note the acantholysis.

Fig. 5.20 Pemphigus foliaceus: multiple erosions are present with background erythema and postinflammatory hyperpigmentation. Courtesy of the Institute of Dermatology, London, UK.