Pemphigus
Pemphigus
Pemphigus (Gr. pemphix, blister) refers to a group of chronic blistering diseases which develop as a consequence of autoantibodies directed against a variety of desmosomal proteins.1–7 The condition as a whole is rare, with an annual incidence ranging from 0.1 to 0.7 per 100 000 of the general population.2 It is more common in the Jewish population, in which the annual incidence rises to 1.6–3.2 per 100 000.7,8 Ashkenazi Jews are the most frequently affected.7,8 The incidence in India also appears to be higher than in other countries.9 There is no sex predilection.
The typical skin lesion is a fragile, flaccid blister, which develops on normal or erythematous skin, and readily ruptures, leaving a painful, crusted, raw, bloody erosion (Figs 5.4 and 5.5). Lesions are most often seen on the scalp, face, axillae, and groin, although in some patients they are generalized (Figs 5.6–5.8).1–3,26 Blisters can be induced by rubbing the adjacent, apparently normal skin – the Nikolsky sign. Direct pressure applied to the center of the blister is also followed by lateral extension – the Asboe-Hansen sign.2 Healing is often accompanied by postinflammatory hyperpigmentation but scarring is not a feature.2
Before the introduction of corticosteroid therapy, the lesions usually became more extensive and in the past often led eventually to death. Treatment with high doses of corticosteroids, immunosuppressants (such as azathioprine), intravenous immunoglobulins, and, more recently, biologicals (such as rituximab) has significantly reduced the mortality to 5–15%, and prolonged remissions without treatment are now being reported.2,27,28 A considerable proportion of the deaths that do occur, however, are due to the side effects of therapy and include staphylococcal infections and, to a lesser extent, pulmonary embolism.2 Severe opportunistic infections due to a wide range of organisms including listeria, nocardia, enterococci, herpes virus, cryptococcus, and candida may further complicate the disease.29–36 Patients may also suffer from Cushing syndrome, adrenal insufficiency, and myasthenia gravis, and appear to have a slightly increased risk of leukemia and non-Hodgkin lymphoma.36
The clinical features and, therefore, classification of these disorders depend on the level of separation within the epidermis:
• In pemphigus vulgaris (p. vulgaris) and pemphigus vegetans (p. vegetans), the blisters are suprabasal.
• In pemphigus foliaceus (p. foliaceus), pemphigus erythematosus (p. erythematosus), and fogo selvagem, the blisters are situated more superficially. P. vulgaris is by far the most common variant, accounting for 80% of cases.7,10,11
In addition to affecting humans, pemphigus has been described in a variety of animals including dogs, cats, goats, and horses.12
Nail involvement seems to be more common than previously reported and may precede skin findings.37 Patients may present with hemorrhagic paronychia, chronic paronychia, trachyonychia, onycholysis, or onychomadesis.21,37–39 Paronychia and onychomadesis are the most common nail changes encountered. Nail involvement is more common in the nails of
172 Acantholytic disorders
Pemphigus variant Autoantigen
Pemphigus vulgaris Dsg3 (mucosal), Dsg1 (cutaneous), desmocollins, pemphaxin, α9- acetylcholine receptor
Pemphigus vegetans Dsg3, Dsc1, and Dsc2 in some patients
Pemphigus foliaceus Dsg1
Pemphigus erythematosus Dsg1
Fogo selvagem Dsg1, rarely also Dsg3
IgA pemphigus Dsc1, Dsg1 or Dsg3
Herpetiform pemphigus Dsg1, rarely also Dsg3
Paraneoplastic pemphigus Desmoplakins I and II, envoplakin, periplakin, BP230, plectin, Dsg1, and Dsg3
Drug-induced pemphigus Dsg1 or Dsg3
Dsc, Desmocollin; Dsg, desmoglein. Modified from Martel, P., Joly, P. (2001) Pemphigus: autoimmune diseases of keratinocyte’s adhesion molecules. Clinical Dermatology, 19, 667.
173 Pemphigus
found, and intact blisters are rare. Exceptionally, the whole mucosa may be affected with subsequent sloughing – esophagitis dissecans superficialis.64,65 Ocular involvement appears to be more common than previously thought, involving up to 26% of patients.66,67 Ocular lesions are usually restricted to the conjunctiva, presenting as conjunctivitis or small vesicles that rapidly rupture.2,66–69 Very rarely, scarring may develop, and corneal ulceration with perforation has been described.70 Vulval, vaginal, and cervical lesions are well recognized and common.71–77 Exceptionally, the vagina may be the sole site of involvement.77 Penile lesions most commonly affect the glans.78,79 They are not usually followed by any significant sequelae.
The development of pemphigus may be associated with a variety of disorders (primarily other autoimmune diseases), including bullous pemphigoid, lupus erythematosus, myasthenia gravis, Hashimoto thyroiditis, vitiligo, minimal change nephropathy, ulcerative colitis, rheumatoid arthritis, and diabetes mellitus.80–88 It has also been described in a patient with the 1p36 deletion syndrome.89 As in many other diseases with an immunological pathogenesis, pemphigus is accompanied by an increased incidence of internal malignancy including thymoma, lymphoma, and multiple myeloma (see paraneoplastic pemphigus).90–93 It has also been reported in association with Kaposi sarcoma.94
digits affected by periungual blisters and also in patients with large number of skin blisters.39
Occasional modes of presentation include linear lesions and pemphigus arising after surgery, burns, vaccination, radiation therapy, and trauma.40–52 Development after exposure to pesticides and an association with cocaine snorting has also been reported.53,54 A very exceptional case has been described in which blisters were initially confined to melanocytic nevi.55 P. vulgaris may also be rarely induced by a variety of drugs, particularly angiotensin-converting enzyme (ACE) inhibitors such as captopril.56–58
In addition to oral and cutaneous involvement, lesions have been described at a wide variety of sites including the nasopharynx, larynx, ear, esophagus, eye, external genitalia, urethra, and anal and colonic mucosa.1,59–61 Esophageal lesions, although originally thought to be rare, have been documented in as many as 63–87% of patients.62,63 Erosions and ulcers are typically
Pathogenesis and histologic features Pemphigus is an immunologically mediated disease.95,96 The most reliable method to confirm the diagnosis is by direct immunofluorescence.97 The later is more accurate than serological methods. Examination of perilesional skin by direct immunofluorescent techniques reveals in vivo-bound immunoglobulin (usually IgG) and often complement (C3) in the intercellular region of the epidermis (Fig. 5.9).98 Abundant antigen in the follicular outer root sheath and germinal matrix may account for the marked scalp involvement typical of pemphigus, and plucked hair follicles may serve as an adequate substrate for direct immunofluorescence analysis.99,100 The in vivo-bound IgG is mainly of the IgG1 and IgG4 subclasses.101
Indirect immunofluorescent techniques show that the serum of patients with pemphigus contains an IgG antibody that reacts with the intercellular region of normal squamous epithelium.102 This antibody is, however, not entirely specific as it may be found in a variety of other conditions, such as severe burns and penicillin drug reactions, and following radiation
174 Acantholytic disorders
referred to as IgG/IgA pemphigus in the literature, this appears to be an ill-defined and heterogeneous disease group.136,139 In addition to p. vulgaris, the additional presence of anti-Dsg IgA antibodies has also been demonstrated in p. foliaceus, p. vegetans, pemphigus herpetiformis, and paraneoplastic pemphigus.136,140,141 Although there is some doubt that this is a truly distinct entity, the so-called IgG/IgA pemphigus may show an atypical clinical presentation with pustules, annular lesions, or a malar rash.139,142–150 Most do not have mucosal involvement.151 Association with malignancy has been suggested.151,152 Histologic features may be more reminiscent of IgA pemphigus, and the presence of IgA antibodies against desmocollins is seen in a subset of patients.139,142–152
The pathogenesis of the acantholysis is uncertain. Direct binding of antibody to the desmosomal cadherins is of major importance and results in internalization of Dsg3 and degradation by the endolysosomal pathway.96,139,153 Plakoglobin has been implicated in mediating intracellular events following IgG binding to Dsg3.154,155 In particular, the role of plakoglobin is signal transduction to the nucleus.154,156 There is also some evidence to suggest that the process may involve, at least secondarily, the action of local proteolytic enzymes.95 The pemphigus antibody induces expression of plasminogen activator receptor on the surface of keratinocytes.157 Binding of plasminogen activator to its keratinocyte cell membrane receptor results in plasminogen activation with resultant production of plasmin.158,159 This latter has non-specific proteolytic activity, which may be responsible at least in part for the dissolution of the desmosomes.96 P. vulgaris antibodies stimulate production of keratinocyte phospholipase C and inositol 1,4,5-triphosphate and increase intracellular calcium. Protein kinase C activation results in release of keratinocyte plasminogen activator and increased expression of plasminogen activator receptor.160–162 Other factors, however, must be of greater importance since p. vulgaris IgG can induce acantholysis in plasminogen activator knockout mice.163 An additional phenomenon is rapid phosphorylation of heat shock protein 27 and p38MAPK, resulting in reorganization and collapse of the cytoskeleton as a result of IgG binding to Dsg3.164,165 This process is mediated by upstream events involving EGF receptor kinase and Src.166 Complement appears not to be essential for acantholysis, and it is thought that any involvement is secondary, perhaps accelerating or extending the process.96 It has been suggested that apoptosis may be induced by p. vulgaris IgG, and that this mechanism may be important in the pathogenesis of the disease.167–169 Other studies have shown that apoptosis is not a prerequisite for blistering and may be a secondary phenomenon.170 Apoptolysis is a process whereby the autoantibodies activate the apoptotic pathway through EGFR/Src signaling through mTOR, resulting in basal cell shrinkage rather than complete apoptosis with subsequent acantholysis.169–171
therapy.103–105 Presumably, pemphigus antigens are released into the circulation following such trauma with resultant antibody production. Circulating antibodies are predominantly of the IgG1 and IgG4 subclasses; IgG3 is identified much less often.106
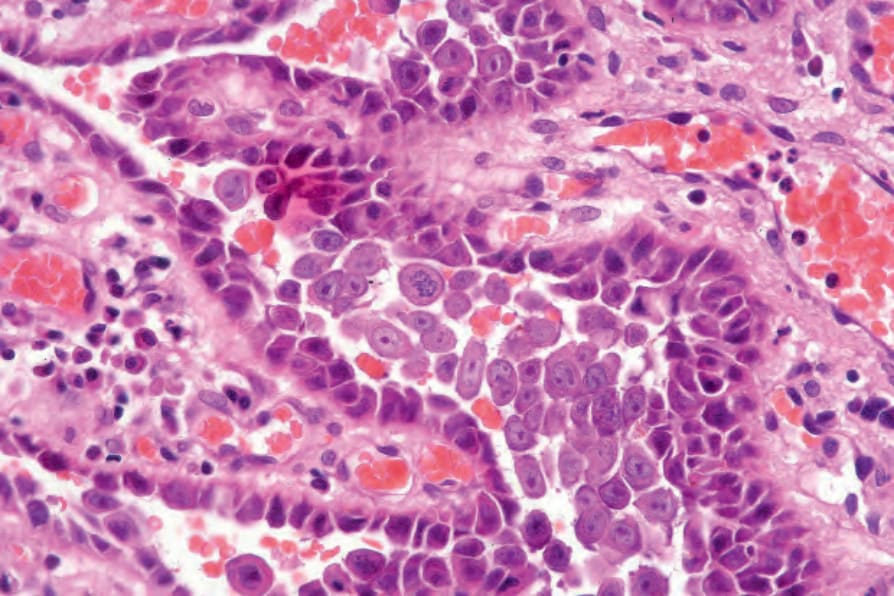
Fig. 5.1 Acantholysis: the keratinocytes are rounded and separated from each other to form an intraepidermal blister. Villi formed from the underlying dermal papillae typically project into suprabasal cavities.
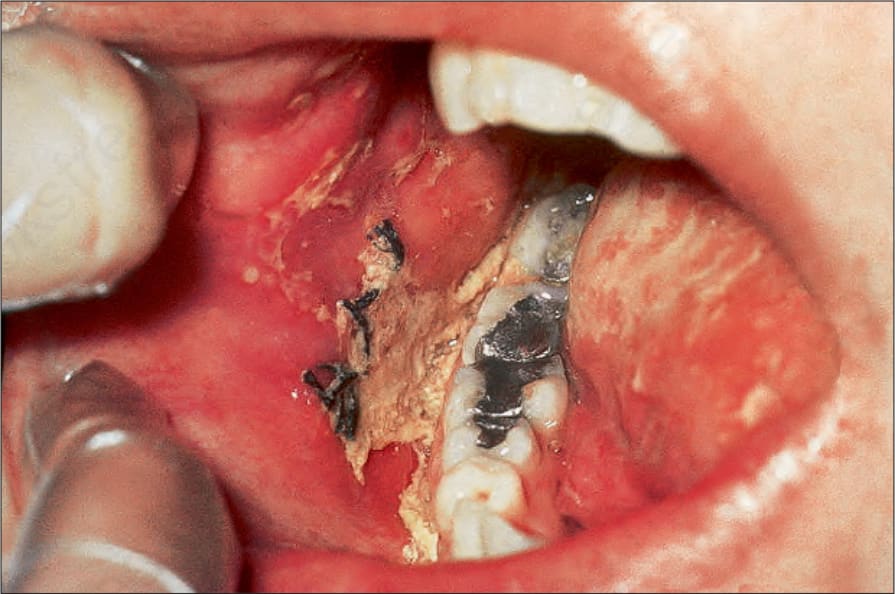
Fig. 5.2 Pemphigus vulgaris: painful erosions are present on the buccal mucosa. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.

Fig. 5.3 Pemphigus vulgaris: in this patient, there is an intact blister on the floor of the mouth. Pemphigus commonly presents in the mouth. By courtesy of the Institute of Dermatology, London, UK.
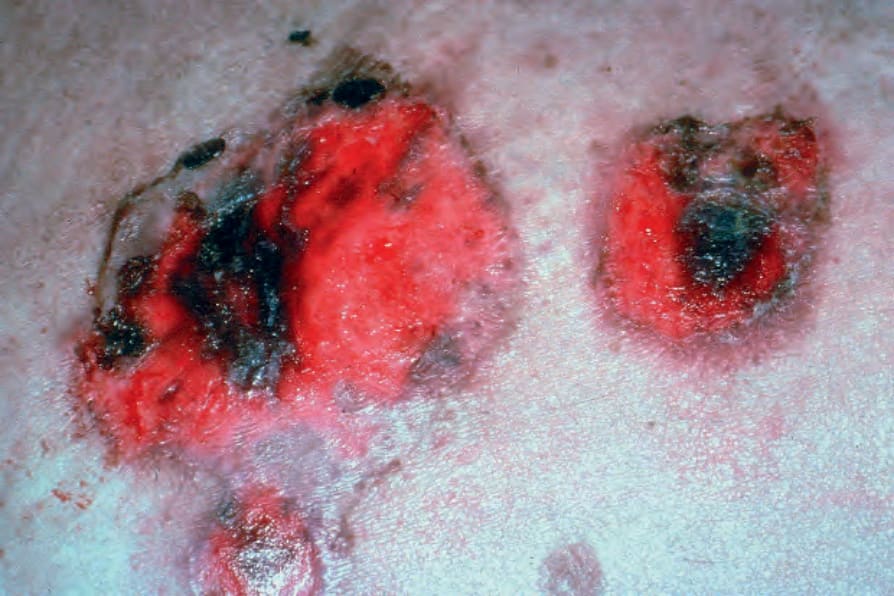
Fig. 5.4 Pemphigus vulgaris: since the blisters are superficial, erosions are more commonly encountered. By courtesy of the Institute of Dermatology, London, UK.

Fig. 5.5 Pemphigus vulgaris: extensive erosions and blisters are present on the shin. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.

Fig. 5.6 Pemphigus vulgaris: umbilical lesions showing intact blisters as well as raw erosions. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.

Fig. 5.7 Pemphigus vulgaris: extensive trauma-induced blisters. By courtesy of the Institute of Dermatology, London, UK.

Fig. 5.8 Pemphigus vulgaris: extensive disease can be very disfiguring. By courtesy of the Institute of Dermatology, London, UK.
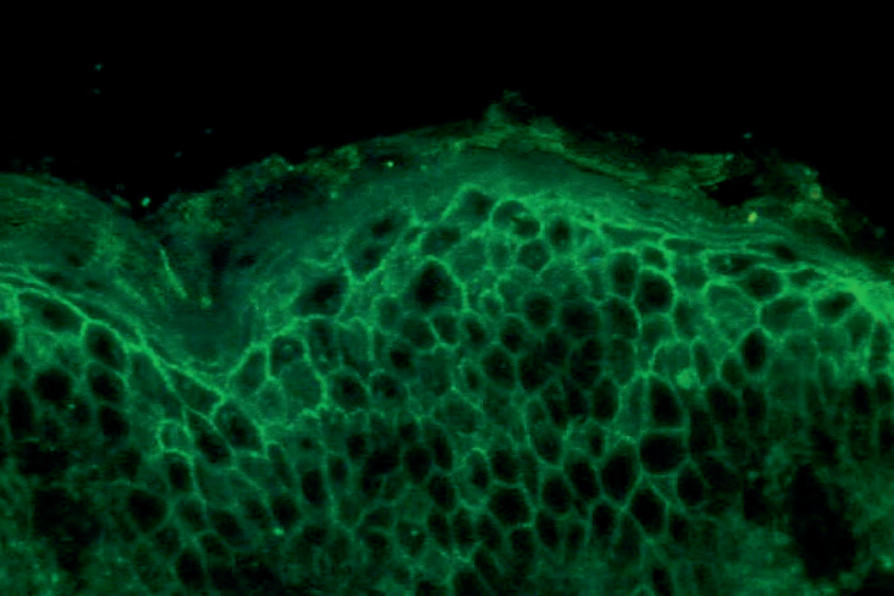
Fig. 5.9 Pemphigus vulgaris: direct immunofluorescence. By courtesy of the Institute of Dermatology, London, UK.
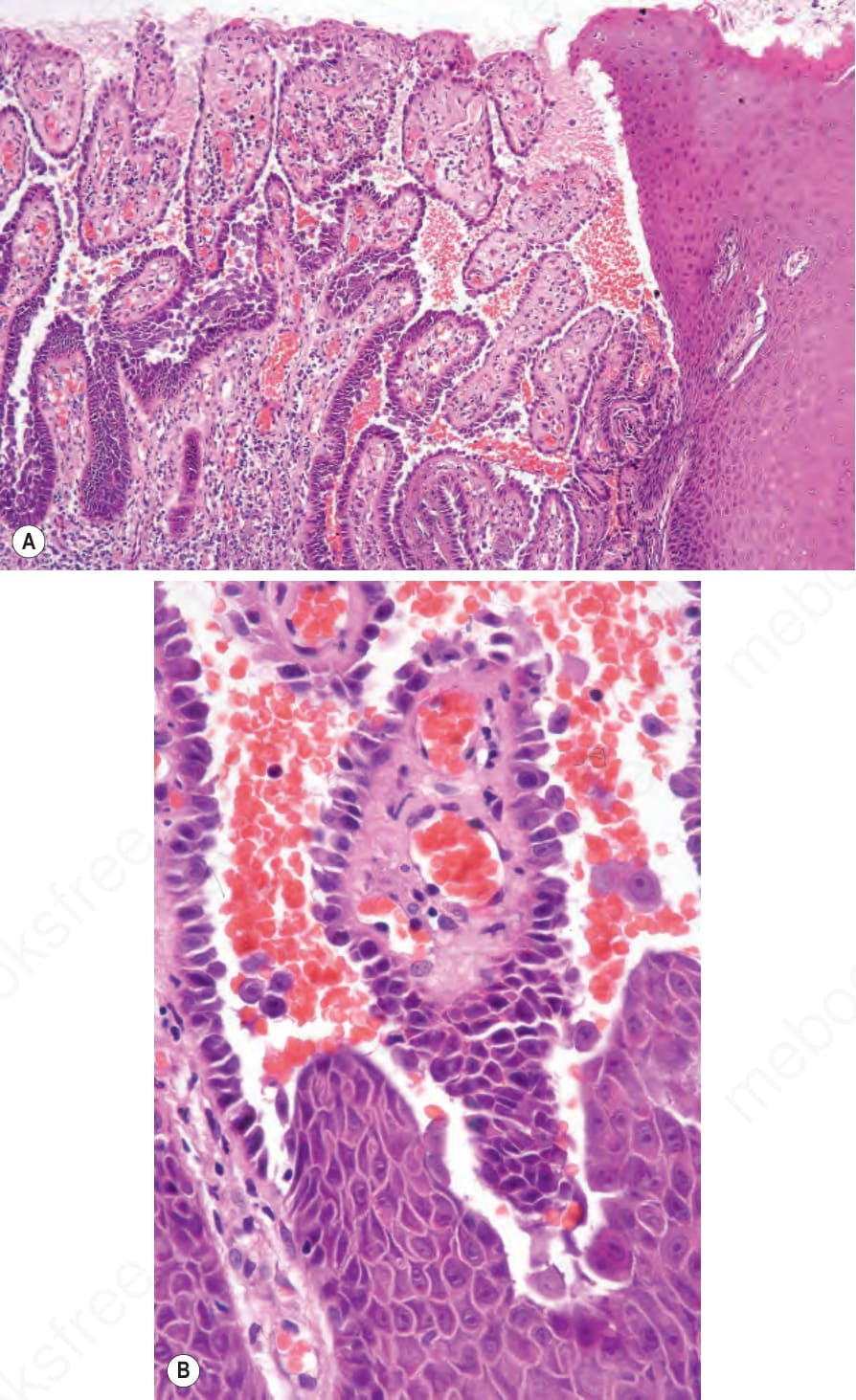
Fig. 5.11 Pemphigus vulgaris: (A) perianal mucosa showing acantholysis and conspicuous villi; (B) high-power view.
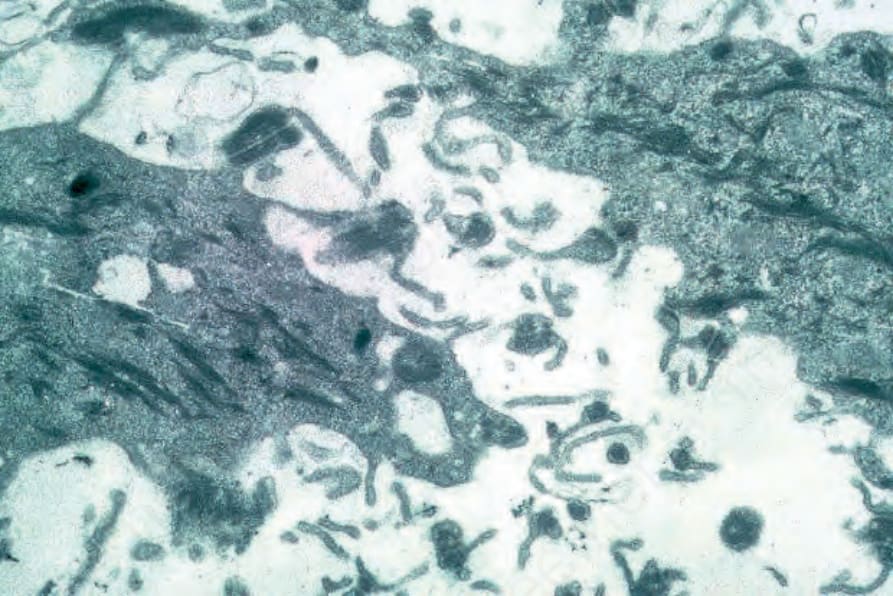
Fig. 5.15 Pemphigus vulgaris: electron photomicrograph of an early lesion showing marked dilatation of the intercellular space. Cytoplasmic ‘villus’ formation is conspicuous and only occasional desmosomes are apparent.
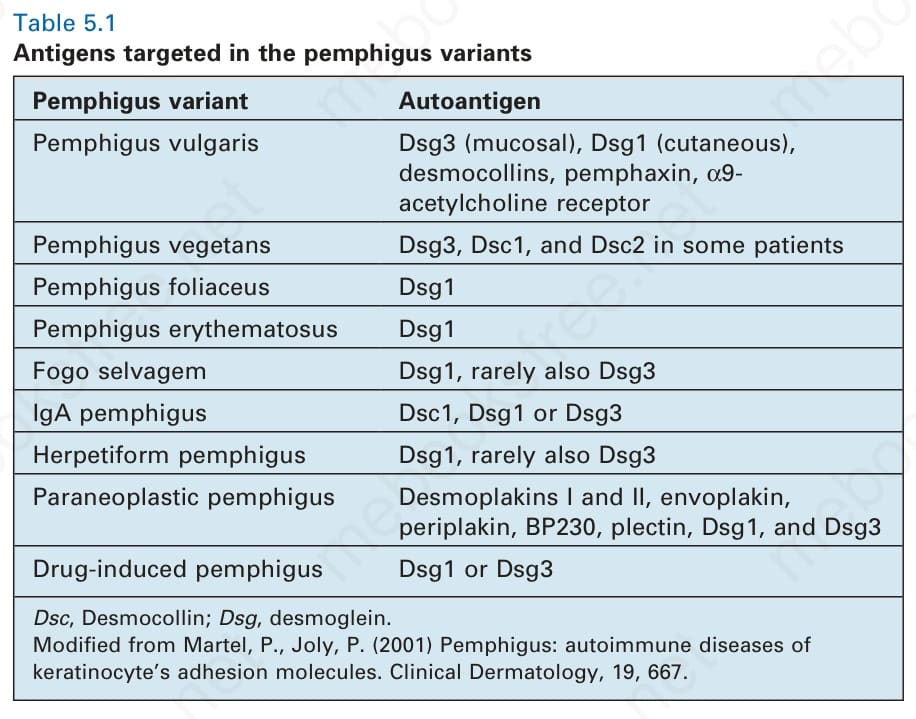
Table 5.1 Antigens targeted in the pemphigus variants
Circulating IgG is pathogenic.96,97 The level of the antibody titer closely parallels the clinical state of the disease.107–110 IgG4 titers diminish during remission whereas circulating IgG1 may continue to be present.97,108 Relapse is commonly preceded by rising IgG4 antibody titers.108
As mentioned above, p. vulgaris rarely may be evident in a neonate born of a mother with active p. vulgaris due to passive transfer of autoantibodies across the placenta.9–15,111,112 The condition is, however, short lived, with lesions disappearing, as the maternal antibodies are catabolized. Passive transfer of IgG4 into neonatal mice results in the development of blisters.112 Purified IgG from pemphigus induces acantholysis in human skin explants and keratinocyte cultures.113,114
The pemphigus antibody binds to the full thickness of the epidermis. Compared with p. vulgaris, immunofluorescence studies on the sera of p. foliaceus patients tend to show more staining in the superficial epidermis, correlating with the level of the split.115,116 Conversely, the sera from patients with p. vulgaris show more affinity for the lower epidermis. Despite these trends, we do not base diagnoses on these (often subtle) differences in immunofluorescence staining distribution.
The p. vulgaris antibody is directed at the extracytoplasmic domain of the 130-kD epithelial desmosomal cadherin, desmoglein 3 (Dsg3), which forms a complex with plakoglobin (85 kD).117–123 The p. vulgaris antibody, however, does not recognize the latter. Many patients also have antibodies that bind to the p. foliaceus antigen, desmoglein 1 (Dsg1), a 160-kD polypeptide.124,125 Dsg3 is expressed primarily in the oral mucosa and, therefore, antibodies directed against this antigen result in mucosal pemphigus. In contrast, Dsg1 is a cutaneous antigen and, therefore, antibodies directed against it result in lesions affecting the skin but not the mucosa (cutaneous pemphigus).115 Anti-Dsg1 antibodies also show cross-reactivity against Dsg4, another member of the desmoglein family.126,127 While patient sera contain antibodies against nonconformational epitopes of Dsg3, active disease correlates with the presence of antibodies directed against the NH2-terminal aspect of Dsg3, in particular ectodomains 2–4.128–130 Oral disease is particularly associated with reactivity to ectodomains 1–4, which is reduced in cutaneous pemphigus.128
T cells are also critical to the development of the antibody-mediated acantholysis.95 CD4+ memory T cells are predominantly involved and both T-helper 1 (Th1) and Th2 Dsg3-specific subtypes are represented.172,173 Th1 T cell-derived interferon-γ stimulates production of IgG1, and Th2 cells produce interleukin (IL)-4 and IL-13, which are responsible for secretion of B cell-derived IgG4.174 Both populations are therefore of importance in stimulating production of p. vulgaris antibody.97 In addition, there is evidence that tumor necrosis factor 1 (TNF-1), Fas-ligand, and IL-1 are also of importance in the development of acantholysis.175 Knockout mice for both these cytokines show diminished acantholysis in passive antibody transfer experiments.176
Antibodies reactive to a number of other proteins including desmoplakin, desmocollins, pemphaxin, and acetylcholine receptor have also been demonstrated in the sera of p. vulgaris patients.130–135
Sera from patients with p. vulgaris not infrequently contain additional IgA antibodies, in particular against Dsg1 and Dsg3.136–138 Although the combination of both IgG and IgA antibodies has, in some instances, been
There is considerable evidence of a genetic background influencing susceptibility to pemphigus as shown by strong associations with human leukocyte antigen (HLA)-DRβ10402, HLA-DRβ11401, and HLA- DQβ1*0503.176–180 Perhaps surprisingly, however, there are only occasional documented reports of familial occurrence.181–184
Pemphigus blisters rupture easily. It is therefore essential to biopsy an early lesion to establish the correct diagnosis.186a The characteristic acantholysis develops because of damage to the intercellular bridges. Acantholytic cells are rounded and have intensely eosinophilic cytoplasm, pyknotic nuclei, and perinuclear halos.185 An early lesion of p. vulgaris shows a slitlike suprabasal cleft or vesicle containing occasional acantholytic cells. The established blister contains acantholytic cells in clumps and in isolation (Figs 5.10 and 5.11). Characteristically, the floor of the cavity is lined by a single
175 Pemphigus
A
layer of intact basal cells, the so-called ‘tombstone’ pattern (Fig. 5.12).152 The acantholytic process frequently involves the epithelium of the adnexae, which can be a useful diagnostic clue in those lesions which lack the roof of the blister (Fig. 5.13).186 Acantholytic changes are also seen in epidermoid cysts. The dermal papillary outline is usually maintained, and frequently, the papillae protrude into the blister cavity. Sometimes the features of eosinophilic spongiosis are seen on biopsy, particularly in early lesions.187 The blister cavity often contains a few inflammatory cells (notably eosinophils), and in the dermis, there is a moderate perivascular chronic inflammatory cell infiltrate with conspicuous eosinophils, although sometimes these are scanty or even absent. Mucous membrane lesions show similar histology.
The histologic features can in part be explained by the compensation theory.120,169 This theory suggests that one Dsg type may be sufficient to maintain epithelium integrity by compensating for the loss of the specific Dsg targeted. In mucosal predominant pemphigus, the autoantibodies target Dsg3, and the relative lack of Dsg1 in mucosa explains the prominent acantholysis in the mucosa and relative sparing of the epidermis. The presence of Dsg1 compensates for the loss of Dsg3 in the skin. In p. foliaceus (see below), the primary target is Dsg1, which is primarily found in the upper epidermis. This explains the superficial nature of the split and sparing of the mucosa, which lacks significant Dsg1.
Ultrastructurally, there is dilatation of the intercellular space with consequent stretching of the desmosomal attachment points (Figs 5.14 and 5.15).188 With progression, these separate and eventually disappear, with residual cell membranes often showing a pseudovillous morphology. Hemidesmosomes are morphologically normal. Immunoelectron microscopy confirms that the immunoreactants are located within the intercellular space.
B
Endemic pemphigus vulgaris Patients with clinical and histologic presentation of p. vulgaris but epidemiological features of fogo selvagem were identified in the Goiania and Brasilia regions of Brazil, known endemic areas of p. foliaceus. These patients demonstrate classical mucocutaneous disease and antibodies to both Dsg1 and Dsg3, but are remarkable for early onset of disease, frequently before the age of 20.189
Differential diagnosis The differential diagnosis of p. vulgaris includes a variety of conditions such as Darier disease, Hailey-Hailey disease, and transient acantholytic dermatosis (Grovers disease) (Table 5.2). In the absence of clinical information or without immunofluorescence studies, it may be impossible to establish a definitive diagnosis. None of these diseases has a specific pattern of immunoreactivity on direct immunofluorescence.
Dyskeratosis in the form of corps ronds and grains is typical of Darier disease, but is rarely seen in Hailey-Hailey disease, and is not a feature of pemphigus. In Hailey-Hailey disease, the perivesicular epithelium is likened to a dilapidated brick wall, an effect sometimes seen in p. vulgaris. More frequently, however, the epithelium overlying and adjacent to the blister is essentially intact.
Acantholysis involving the follicular epithelium is often seen in pemphigus, but usually not in Hailey-Hailey disease. The pemphigus-like variant of Grover disease is histologically indistinguishable from pemphigus, but the clinical history, minute size of the lesions as viewed by the microscope, and negative immunofluorescence findings make distinction relatively easy. Extreme degrees of acantholysis in acantholytic solar keratosis may on rare occasions be confused with the previously mentioned acantholytic disorders. Similarly, it is important not to misinterpret the trivial finding of incidental focal acantholytic dyskeratosis in a skin specimen removed or biopsied for an unrelated finding.
176 Acantholytic disorders
Pemphigus vulgarisa Darier diseasea
Hailey-Hailey diseasea
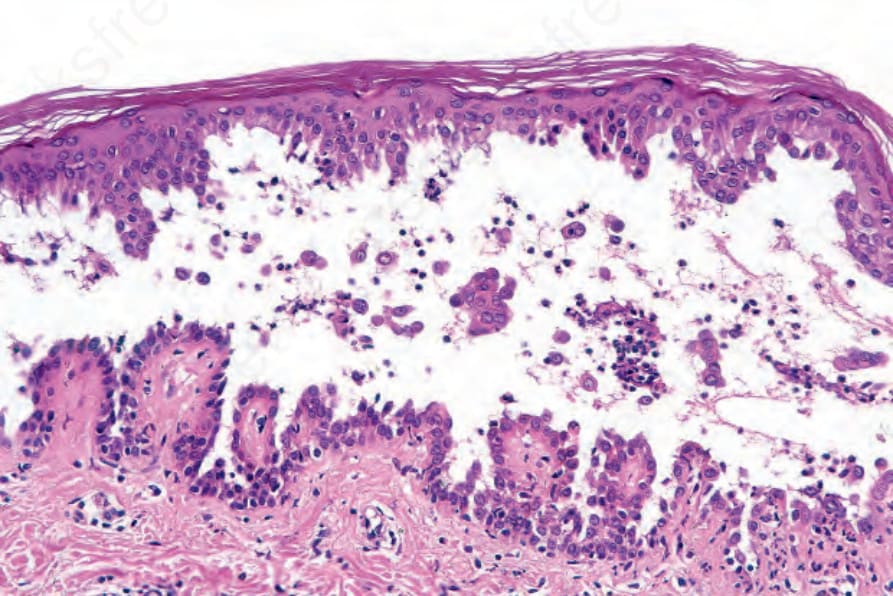
Fig. 5.10 Pemphigus vulgaris: established blister showing marked acantholysis and scattered neutrophils. The dermal papillae project into the cavity as villi.
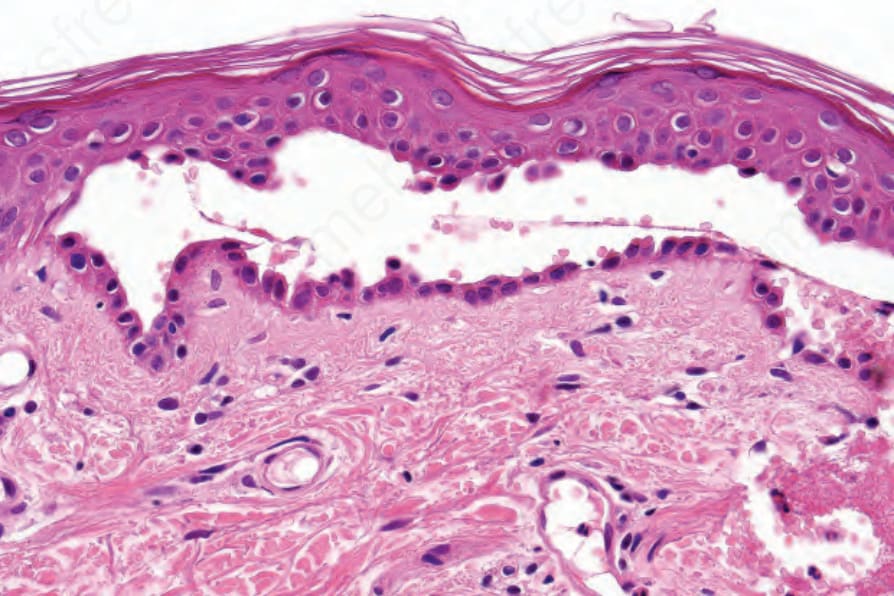
Fig. 5.12 Pemphigus vulgaris: cell-free example showing a linear palisade of intact basal keratinocytes – the so-called ‘tombstone’ appearance.
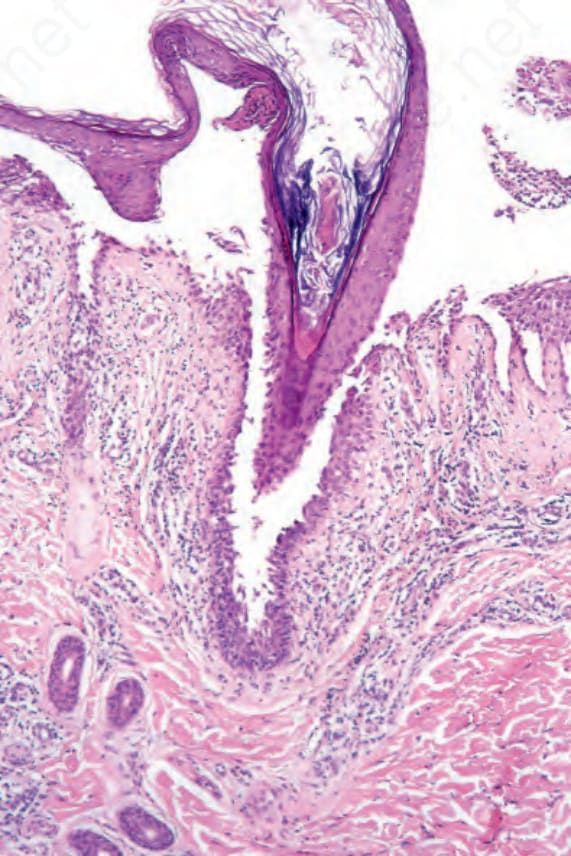
Fig. 5.13 Pemphigus vulgaris: follicular involvement distinguishes pemphigus from Hailey- Hailey disease in which it is not a feature.
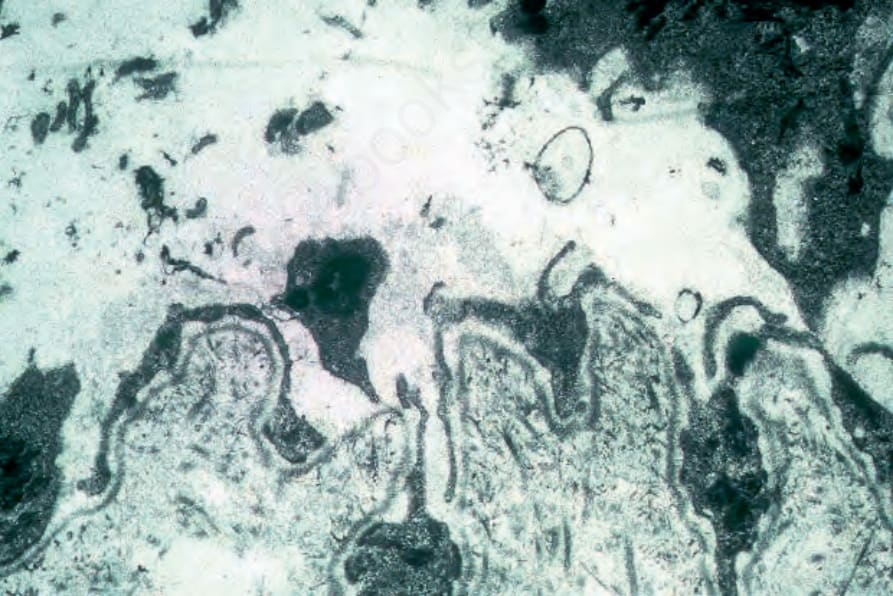
Fig. 5.14 Pemphigus vulgaris: electron photomicrograph of an early lesion showing suprabasal, intraepidermal vesiculation. Residual cytoplasm of basal keratinocytes lines the floor of the blister. The lamina densa is clearly visible.
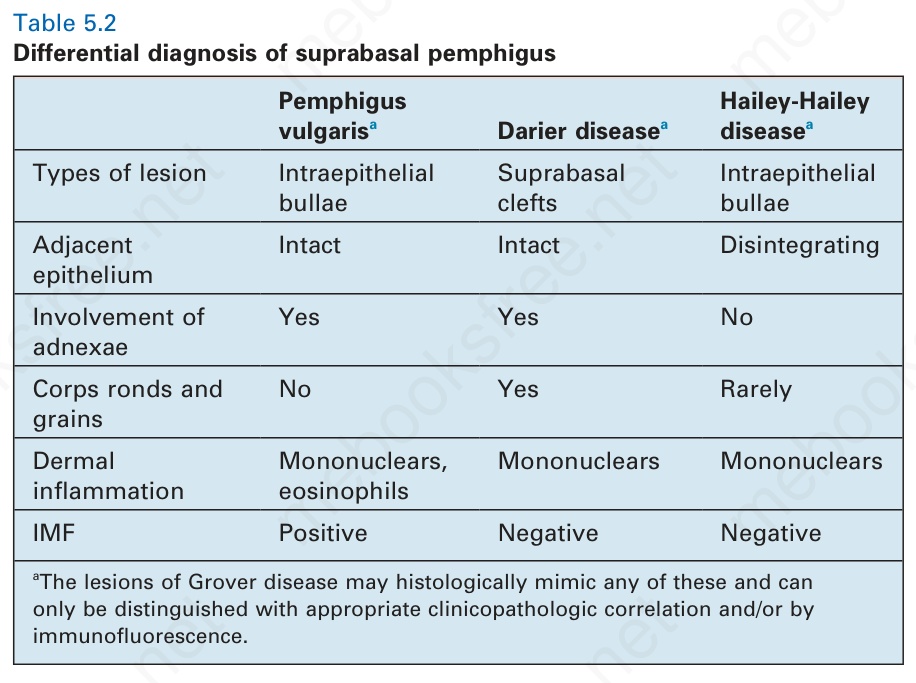
Table 5.2 Differential diagnosis of suprabasal pemphigus