Pemphigoid gestationis
Pemphigoid gestationis
Pruritus is a very common symptom in pregnancy, occurring in up to 18% of gravid females.1–4 When it occurs in the absence of significant cutaneous stigmata it is known as pruritus gravidarum. This may occasionally be associated with a cholestatic pathogenesis. The specific pregnancy eruptions have long been a source of considerable confusion and controversy in the literature, largely due to a diverse range of terminologies and classifications. Holmes has attempted to clarify the situation with the introduction of a new and much simplified classification and others have proposed similar schemes.2,5 Therefore the specific dermatoses of pregnancy may be divided into:
• polymorphic eruption of pregnancy, where the predominant lesions are urticarial; in the United States, the term pruritic urticarial papules and plaques of pregnancy (PUPPP) has achieved greater popularity;
• pregnancy prurigo in which the lesions consist of itchy papules;
• pemphigoid (herpes) gestationis, an autoimmune dermatosis belonging to the bullous pemphigoid group of diseases. Pemphigoid gestationis is a bullous dermatosis of pregnancy and the puerperium. It may be exacerbated by the use of oral contraceptives and rarely complicates hydatidiform mole and gestational (but not nongestational) choriocarcinoma. The current evidence implicates an autoimmune-mediated pathogenesis in which hormonal influences play a significant role.6,7
Pemphigoid gestationis usually complicates subsequent pregnancies, frequently presenting earlier on and with more severe symptomatology.10 Sometimes, however, it may skip intervening pregnancies.3 This may be related to a change in paternity, or else due to compatibility at the HLA-D locus.
Pemphigoid gestationis may develop into a very protracted ‘postpartum’ illness associated with considerable morbidity and lasting up to 12 years.17,18 In the majority of patients, however, the disease resolves by about 6 months postpartum.4 The disease may first present following a change in sexual partner.3,19 Alternatively, recurrent disease may persist even when there has been a change of sexual partner.7 This obviously calls into question the role of specific paternal antigens.
Exacerbation following the use of the oral contraceptive is a common complication,10,20–23 affecting 20–50% of patients.3 Estrogens in particular have been implicated.22 The condition may also relapse during menstruation for some weeks or months postpartum and the return of symptoms (pruritus) has also been noted to coincide with ovulation (again suggesting an estrogen influence), although this is rare.3,10,22
Clinical features The term herpes (gestationis) is neither appropriate nor satisfactory. It is not of viral etiology, nor has it anything to do with creeping (Gr. herpes, to creep). It was originally so named because of the tendency of the disease to show ‘progressive involvement by peripheral extension’.3 Because of its intimate relationship to bullous pemphigoid, the designation pemphigoid gestationis is preferred. As the major larger series have consisted of patients derived from a variety of sources, estimates of incidence have been very variable, ranging from 1 : 3000 to 1 : 50 000 pregnancies.4,8–10 A further study
Evidence has been published relating the duration of symptoms postpartum to the practice of breast-feeding. Bullous lesions lasted only 5 weeks in those who breast-fed compared to 24 weeks in those who bottle-fed. Although hormonal factors must be implicated, the precise pathogenetic implications underlying this observation are not fully understood.22
Pemphigoid gestationis is associated with intense pruritus, which may be present for days or weeks before the onset of typical cutaneous manifestations.1 The dermatosis is characteristically polymorphous, consisting of erythematous or urticarial papules and plaques, some with a polycyclic pattern, and later vesicles and bullae develop at the periphery of spreading erythematous plaques (Fig. 4.77).3,10,24 When fully evolved, the blisters are tense and contain clear fluid, but at times the fluid may become hemorrhagic (Fig. 4.78). They typically heal without scarring.
146 Inherited and autoimmune subepidermal blistering diseases
The umbilicus is frequently the site of initial involvement; spread to the trunk and extremities then follows (Figs 4.79 and 4.80).3 Surprisingly, lesions on the face and mucous membranes are distinctly uncommon. Eventually palmar and plantar manifestations may appear. Other than pruritus, symptoms are usually mild, with stinging, burning, and pain being relatively infrequent.10 Occasionally, the presence of target or iris lesions may mimic erythema multiforme.25 Less commonly, features may initially suggest classical bullous pemphigoid.25 Very occasionally, there is clinical overlap with dermatitis herpetiformis.
Pemphigoid gestationis is not associated with pre-eclamptic toxemia and there is no related maternal mortality.
Pemphigoid gestationis is accompanied by a significant increased risk of developing Graves disease, thyroiditis, pernicious anemia and an increased risk of autoantibodies,26 likely reflecting the association of HLA-DR3 and HLA-DR4 loci with both pemphigoid gestationis and autoimmune disease.26
The literature concerning the incidence and nature of fetal morbidity and mortality is a source of some confusion. Kolodney therefore considered that there was no evidence of an increased incidence of stillbirths or abortions; however, his report predates the immunofluorescence era.5 An investigation by Lawley et al.20 of a large series of cases where immunofluorescent confirmation was available, suggested that there was an increased risk of fetal morbidity and mortality. More recently, evidence has been presented that patients with pemphigoid gestationis are liable to deliver low weight and small-for-dates infants, prematurely.27 In contrast, however, Shornick et al. failed to show any evidence of significant fetal complications.7 It has been shown that the onset of the disease in the first and second trimester and the presence of blisters is associated with higher morbidity including premature birth and low birth weight children.28 Morbidity, however, still remains low.
The antibody can cross the placenta and, in approximately 5% of cases, this may be associated with a mild and transient vesiculobullous eruption.29–32
Pathogenesis and histologic features The histopathologic features seen in biopsies from patients with pemphigoid gestationis are variable, depending upon whether early erythematous lesions, urticarial papular lesions, or fully established vesicles and bullae are studied.33
In early lesions, the major pathological features are seen in the superficial dermis where there is a perivascular inflammatory cell infiltrate consisting of lymphocytes, histiocytes, and typically very large numbers of eosinophils. This is associated with edema of the papillary dermis, which when marked may result in a ‘teardrop’ appearance (Fig. 4.81).33 Sometimes there is accompanying spongiosis and this may be associated with large numbers of eosinophils (eosinophilic spongiosis, Fig. 4.82). Occasionally the infiltrate of lymphocytes, histiocytes, and eosinophils is present in a linear distribution along the dermal–epidermal junction.3
147 Pemphigoid gestationis
dermis is edematous and contains a predominantly perivascular lympho/ histiocytic infiltrate with large numbers of eosinophils. Leukocytoclasis and eosinophil dermal papillary microabscesses are only rarely identified.33,34 Ultrastructural studies show that the cleavage plane lies within the lamina lucida.33,35
Direct immunofluorescence of perilesional skin in pemphigoid gestationis shows a linear basement membrane zone deposition of C3 in all patients.3,36–41 About 30–50% of cases also have an IgG band (less frequently IgM or IgA).36 They are present in nonlesional (perilesional) as well as in lesional skin.36 It has been suggested that demonstration of linear C3d deposition at the dermal–epidermal junction may be a useful tool in the diagnosis of the disease.42 The authors of this study used immunohistochemistry in paraffin-embedded, formalin-fixed material with good results. Complement pathway components including properdin and properdin factor-B may also be identified.1 IgG and complement can often be detected along the amniotic basement membrane region using direct immunofluorescence.38,43,44 Pemphigoid gestationis antigen has been detected in the placenta from early in the second trimester onwards.45 The antibody may also be found in the skin of infants of affected mothers.29 Interestingly, serologic evidence of pemphigoid gestationis without manifestation of the disease may be seen. An exceptional case of neonatal pemphigus in a child whose mother had clinical and serologic evidence of pemphigus vulgaris but only serologic evidence of pemphigoid gestationis has been described.46
Vacuolar degeneration of basal keratinocytes, sometimes accompanied by individual cell necrosis, may be a feature of the early lesions, but is often more evident in the fully established vesicular or bullous stage.33 In the latter, the blister is subepidermal in location and frequently contains large numbers of eosinophils (Figs 4.83 and 4.84).33 The underlying and adjacent
148 Inherited and autoimmune subepidermal blistering diseases
Circulating complement-fixing (via the classical pathway) IgG antibodies (pemphigoid [herpes] gestationis [HG] factor) can be detected in 50–75% of cases by indirect complement immunofluorescence (Fig. 4.85).20,36,47–51 The so-called HG factor is nothing more than a low titer IgG complement-fixing antibasement membrane antibody.36 The antibody can be of any IgG subclass; IgG1 and IgG4 have been reported as predominant.38,51 If monoclonal antibodies directed against IgG are used, 100% of patients can be shown to possess circulating HG factor.38 Approximately 25% of patients have antibasement membrane zone antibodies detectable by conventional techniques.51 These bind to the roof of 1 M NaCl-split skin.36 The antibody also reacts with amnion and chorion basement membrane.42,44 The autoantibodies in the disease are directed against collagen XVII which is the BP 180-kD protein (BPAG2). The latter plays a major role in cell adhesion and signaling. It has been demonstrated that collagen XVII is present in the epithelial cells of the amniotic membrane and in syncytial and cytotrophoblastic cells.52 Although the exact pathogenetic mechanism of the disease is still unknown (see below), the presence of collagen XVII in these tissues seems to play a major role in the mechanism of the disease.

Fig. 4.77 Pemphigoid gestationis: prebullous phase showing erythema and small papules. By courtesy of the Institute of Dermatology, London, UK.

Fig. 4.78 Pemphigoid gestationis: the blisters are tense and dome-shaped. By courtesy of R.C. Holmes, MD, Warneford Hospital, Oxford, UK.

Fig. 4.79 Pemphigoid gestationis: slightly raised erythematous lesions with a propensity to cluster on the abdomen. By courtesy of R.C. Holmes, MD, Warneford Hospital, Oxford, UK.

Fig. 4.80 Pemphigoid gestationis: umbilical involvement is a common mode of presentation. By courtesy of the Institute of Dermatology, London, UK.
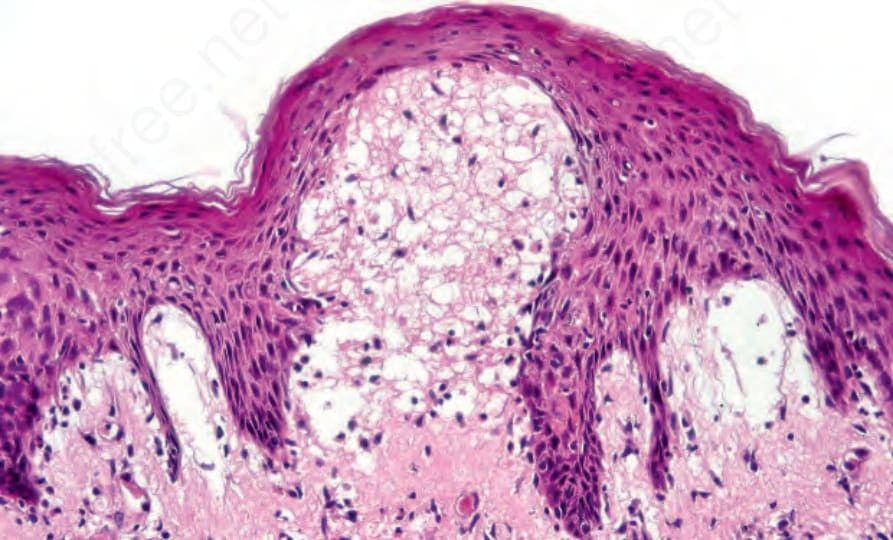
Fig. 4.81 Pemphigoid gestationis: early erythematous lesion showing marked edema of the papillary dermis and conspicuous eosinophils.
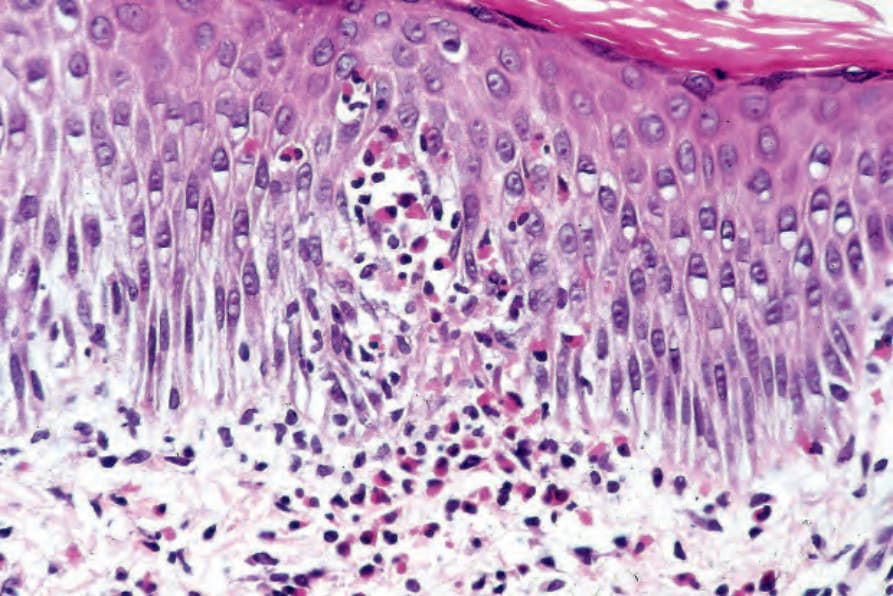
Fig. 4.82 Pemphigoid gestationis: early erythematous lesion showing eosinophilic spongiosis.
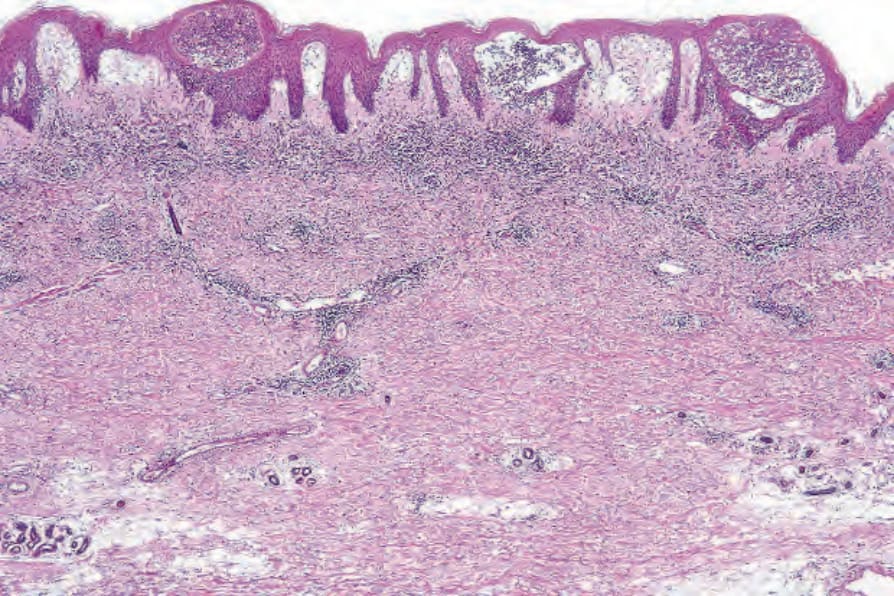
Fig. 4.83 Pemphigoid gestationis: established subepidermal blister.
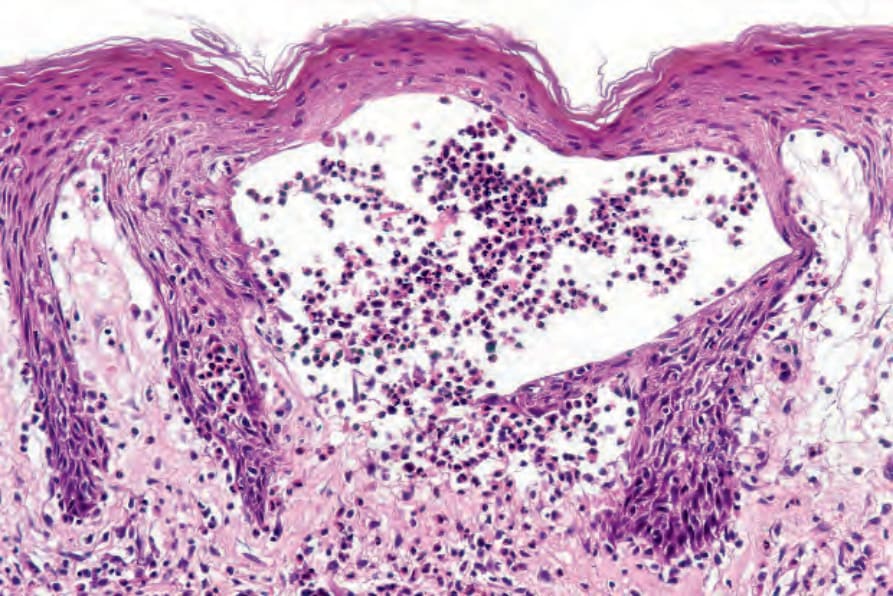
Fig. 4.84 Pemphigoid gestationis: the blister cavity contains a heavy eosinophil infiltrate.
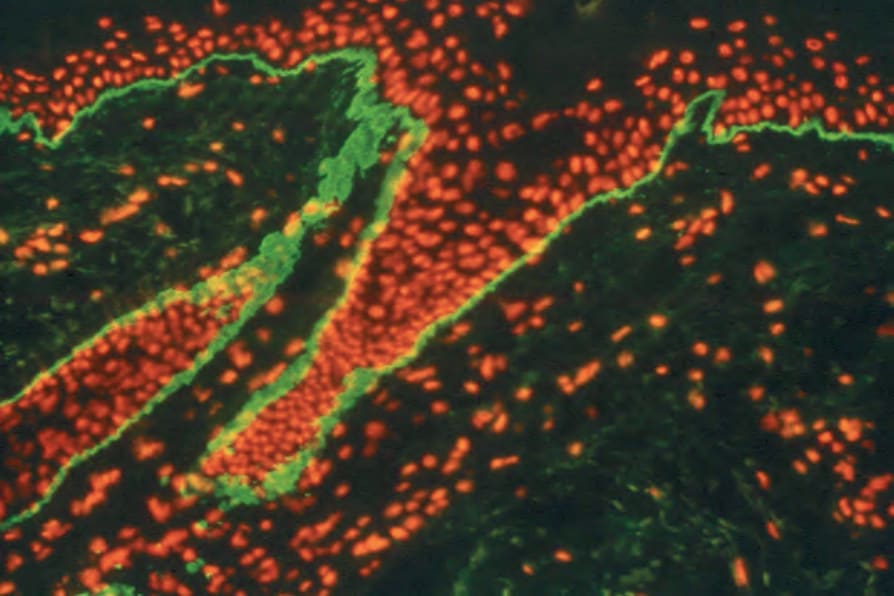
Fig. 4.85 Pemphigoid gestationis: indirect complement immunofluorescence showing linear deposition of IgG.
The presence of pemphigoid gestationis antigen in both skin and amnion raises the possibility that an initial antiplacental antibody cross-reacts with skin, giving rise to the clinical features of pemphigoid gestationis.29 Support for this theory has been the discovery that the HLA antigens -DP and -DR are consistently expressed in the placentas of patients with this condition.64,67 The main antigen present in both the skin and placenta seems to be collagen type XVII and this, associated with genetic predisposition and specific HLA genotype, appears to trigger the disease.68
Differential diagnosis The differential diagnosis includes epidermolysis bullosa acquisita, dermatitis herpetiformis, linear IgA disease, and bullous systemic lupus erythematosus (see Table 4.6). Pemphigoid gestationis must also be distinguished from pruritic urticarial papules and plaques of pregnancy (PUPPP) and pregnancy prurigo.
With immunoelectron microscopy the immunoreactants are deposited within the upper lamina lucida where they are most probably associated with the sub-basal dense plate.53,54 In pemphigoid gestationis the antibody recognizes BPAG2 (collagen type XVII) on Western immunoblot and localizes to the same NC16A domain as described in bullous pemphigoid.55–62 This can be detected in serum using the same test employed for bullous pemphigoid.60–62 Antibodies that recognize the 230-kD bullous pemphigoid antigen are present in 10–26% of cases.56,57 Experimental models indicate that antibodies against the NC16A domain of BP180 are the pathogenic antibodies in pemphigus gestationis just as they are for bullous pemphigoid.7,62 Serum BP180 antibody levels have been demonstrated to correlate with the disease activity and can serve as an indicator for assessment of treatment response.60
PUPPP is predominantly a disorder of first pregnancies. Lesions particularly develop around abdominal striae, and periumbilical sparing is a characteristic feature (Fig. 4.86). Eosinophilic spongiosis and subepidermal blistering may be seen in established lesions and therefore, in the absence of clinical details and immunofluorescence findings, distinction from pemphigoid gestationis may be impossible. Immunohistochemistry for C4d and C3d on formalin-fixed paraffin-embedded tissue can aid in the distinction between PUPPP and pemphigoid gestationis. The majority of pemphigoid gestationis cases display a linear pattern of staining along the basement membrane zone, while in cases of PUPP staining consistently negative.42,69
Pregnancy prurigo, which typically develops in the third trimester, presents with pruritic papules and nodules (Fig. 4.87). Blisters are not a feature. Histologically, the changes are those of a low-grade, non-specific spongiotic dermatitis.
Patients with pemphigoid gestationis have an increased incidence of HLA-B8 (43–79%), HLA-DR3 (61–80%) and HLA-DR4 (52–53%). The paired haplotypes HLA-DR3 and -DR4 are present in 54% of patients compared with 3% in the general population.1,3,22,63,64 The phenotype, however, does not appear to correlate with the clinical features of pemphigoid gestationis.3,65 Patients with pemphigoid gestationis also have a high incidence (100%) of anti-HLA cytotoxic antibodies, particularly directed against the paternal antigens.36,63–66 These are, however, found in 25% of normal multiparous women and therefore their possible role in the pathogenesis of pemphigoid gestationis is uncertain.26
The pathogenesis of pemphigoid gestationis relates to antibody-associated complement fixation with the production of leukocyte chemotactic factors, mast cell degranulation, and associated dermal–epidermal separation.36

Fig. 4.86 Pruritic papules and plaques of pregnancy: note the erythematous papules particularly related to the abdominal striae, and characteristic umbilical sparing. By courtesy of R.C. Holmes, MD, Warneford Hospital, Oxford, UK.

Fig. 4.87 Pregnancy prurigo: there are erythematous papules and excoriations. Blisters are not a feature of this condition. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.
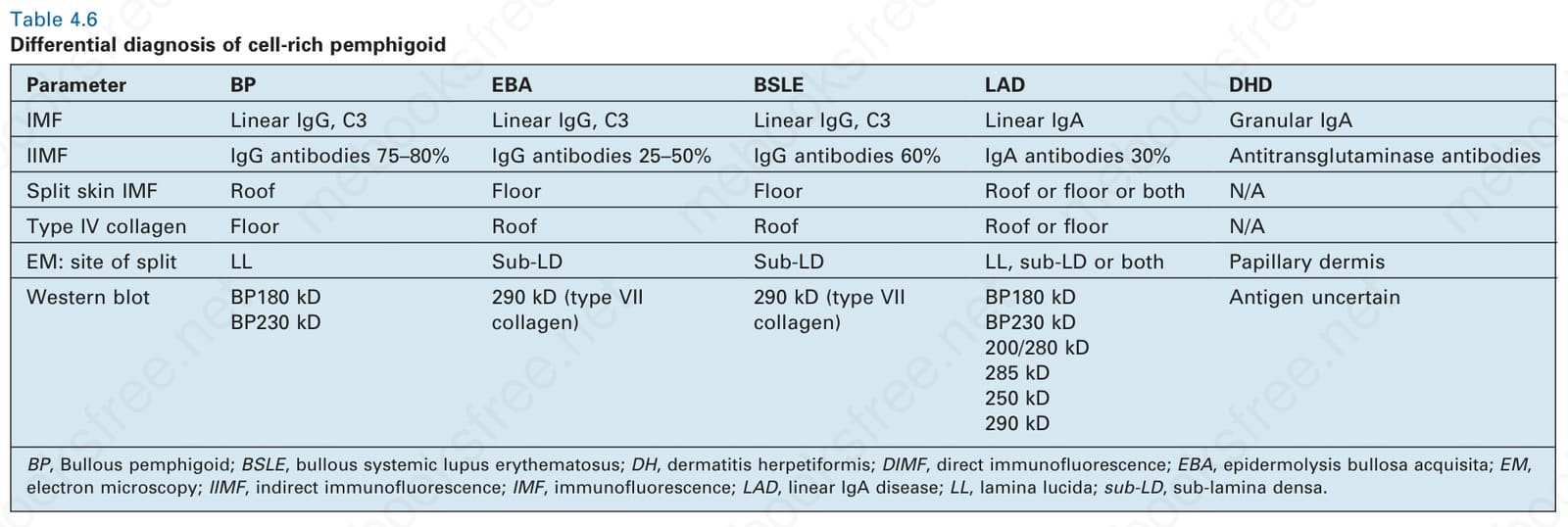
Table 4.6 Differential diagnosis of cell-rich pemphigoid