Digitate hyperkeratosis
Digitate hyperkeratosis
but it also involves other intertriginous areas including submammary and intermammary skin, groins, vulva, perianal region, and, less commonly, nonintertriginous skin including the lower back, buttocks, and flanks.5–8 Women are affected more commonly than men. The disease mainly affects the middle aged to elderly; children are rarely involved and only one congenital case has been reported.8–11 It presents as pruritic or burning erythematous, hyperpigmented, and hyperkeratotic patches, papules, or plaques (Fig. 3.156). Fissures and a ‘cobblestone’ appearance may be seen. The condition has been documented to respond to retinoids and to calcipotriene and ammonium lactate.12,13
Many different hyperkeratotic conditions have been described under names such as minute and filiform keratoses, multiple minute digitate hyperkeratosis, minute aggregate keratoses, digitate keratoses or disseminated spiked hyperkeratosis.1–4 An approach to classification proposed the unifying term multiple minute digitate hyperkeratosis.5 Caccetta et al. proposed a useful algorithm for differentiation.6 Myriad nonfollicular spiky keratoses develop on the trunk and limbs early or late in life and have a transient or persistent course.6Pathogenesis and histologic features
Familial cases of digitate hyperkeratosis have been described with a probable autosomal dominant mode of transmission.2,3,7,8 Acquired cases may be associated with drugs, Crohn disease, and malignancy, including hematological neoplasia and radiotherapy.4,5,8–13 Hyperkeratotic spicules on the face, particularly on the nose, are follicular and often associated with paraproteinemia, multiple myeloma, and cryoglobulinemia, but may also be idiopathic.10,11 Filiform keratoses occur with a pityriasis rubra pilaris-like eruption and acne conglobata in association with HIV infection.14 A familial form of filiform keratosis has been described and is associated with thickened nails, plantar hyperkeratosis, joint laxity, and long fingers (Fig. 3.154).15
Pathogenesis and histologic features The etiology is unknown. It has been suggested that the condition develops as a result of a contact reaction to an antiperspirant or as a result of excessive use of other topical products, including creams, shampoos, and soaps.1–6,8 However, this does not explain the involvement of areas away from the axilla. The molecular mechanism proposed to explain the disease consists of a failure to transform profilaggrin to filaggrin which interferes with the degradation of keratohyalin granules.1,7
The histologic appearance typically consists of a massive hyperkeratosis with parakeratosis and retention of keratohyalin granules in the stratum corneum (Fig. 3.157). The underlying epidermis may show mild acanthosis or even some degree of thinning. Hair infundibula and eccrine ostia are occasionally affected.14,15 Necrotic areas with exocytosis of neutrophils or perforation of the epidermis are rarely found. The superficial dermis contains a sparse perivascular lymphocytic infiltrate.1–7
Histologically, there are compact orthohyperkeratotic spicules mostly arising from a pointed epidermal elevation (Fig. 3.155). The stratum granulosum is usually prominent and parakeratosis may be present.6,15–17 Hyperkeratotic spicules associated with paraproteinemia reveal eosinophilic inclusions that represent immunoglobulin deposits.10
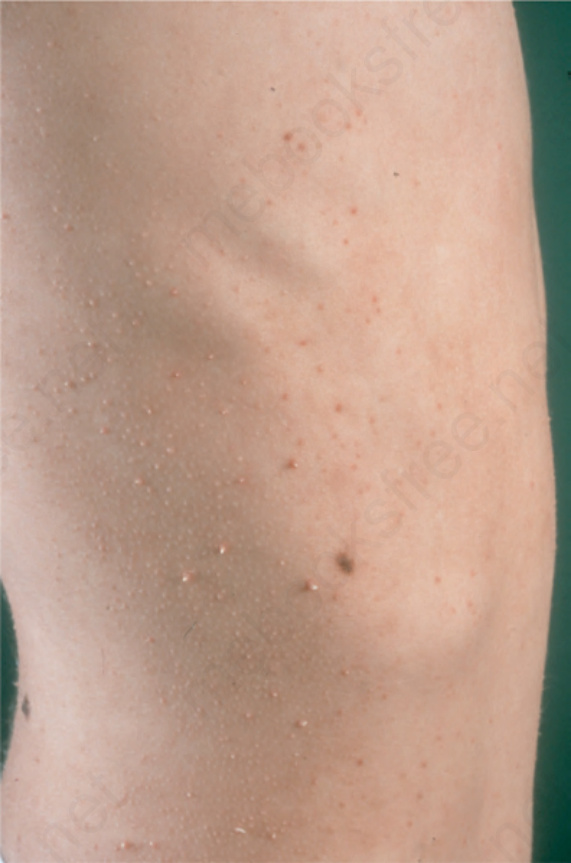
Fig. 3.154 Digitate hyperkeratosis: in this familial variant disseminated spiny keratosis developed on trunk and extremities. By courtesy of H. Traupe, Münster, Germany.
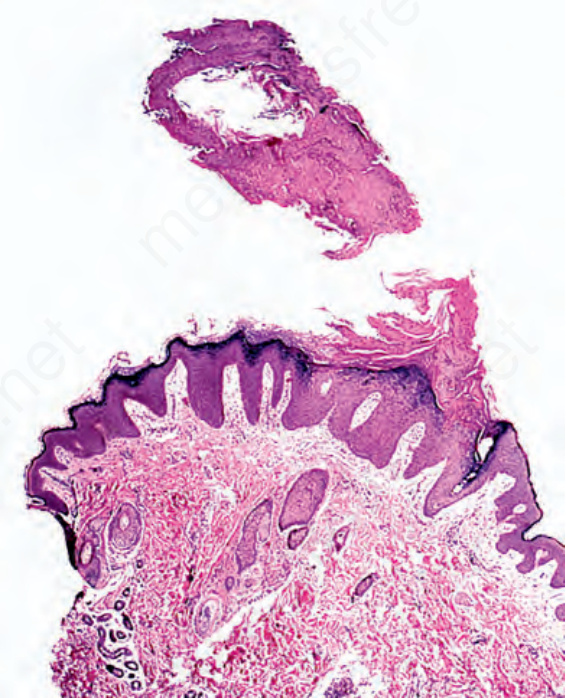
Fig. 3.155 Digitate hyperkeratosis: an orthohyperkeratotic spicule arises from a pointed epidermal elevation.
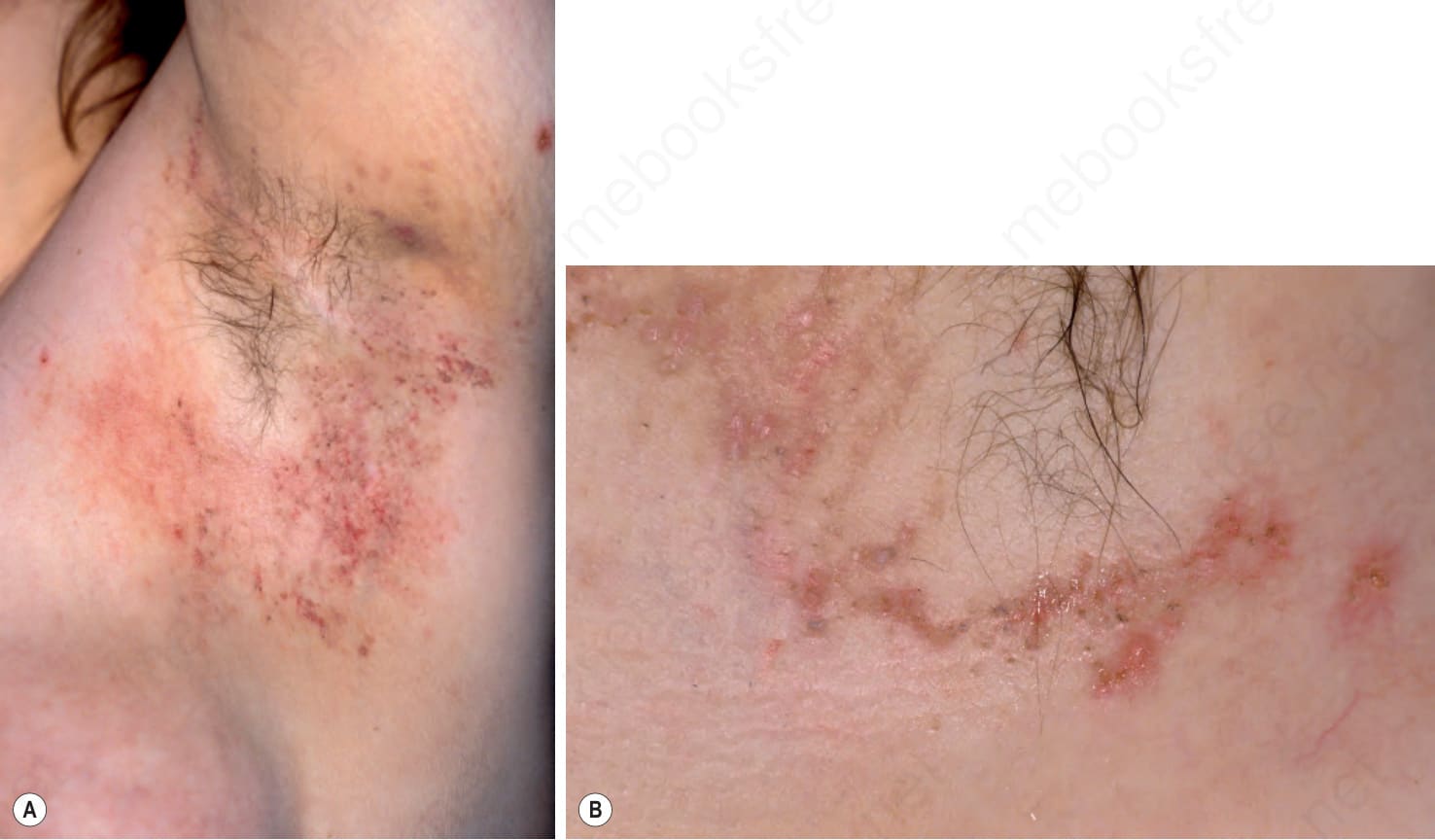
Fig. 3.156 Granular parakeratosis: (A) in the axilla of a middle-aged woman erythematous, hyperpigmented and hyperkeratotic papules develop in a reticulated fashion; (B) a few of these lesions are erosive.
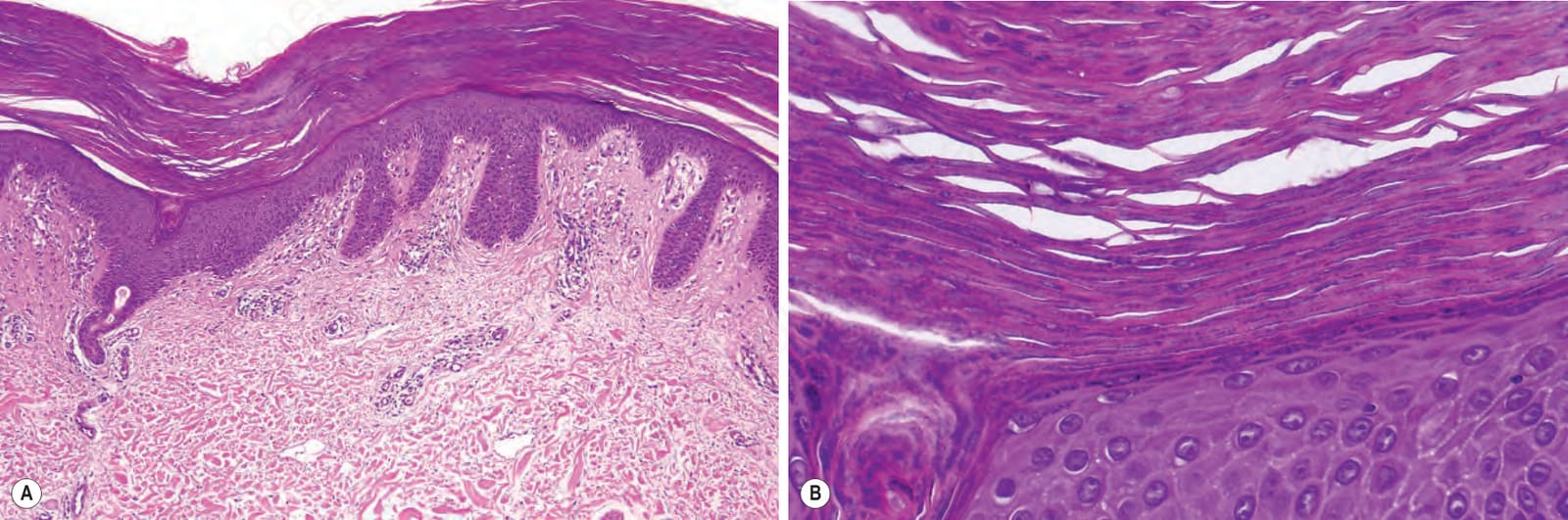
Fig. 3.157 Granular parakeratosis: (A) there is marked thickening of the horny layer with parakeratosis; (B) high-power view showing retention of keratohyalin granules.