Porokeratosis
Porokeratosis
Clinical features Porokeratosis is a heterogeneous group of keratinization disorders, most of them with an autosomal dominant inheritance characterized by a so-called ‘cornoid lamella’. This is a grooved keratotic ridge, from the center of which a keratotic core (cornoid lamella) projects at an obtuse angle that borders
111 Acquired palmoplantar keratoderma and malignancies
A
B
The terms ‘porokeratosis punctata palmaris et plantaris’ or ‘porokeratotic PPK’ should be avoided as they are also used as synonyms for spiny keratoderma (palmoplantar keratoderma punctata, type 2) that is histologically unrelated to porokeratosis.11
In linear porokeratosis, the lesion is clinically reminiscent of an epidermal nevus, involves the extremities, and usually presents in infancy or early childhood (Fig. 3.148).3 A zosteriform variant has also been described.12 Nails may show fissures and pterygium.13 The coexistence of linear porokeratoses and DSAP can be explained by loss of heterozygosity in type 2 of segmental distribution of autosomal dominant disorder.14,15
a pigmented or reddish atrophic center.1–3 Dermoscopy, in particular when using polarized or UV-light, and in-vivo reflectance confocal microscopy, allow visualization of the cornoid lamella.4,5 However, in punctate porokeratosis the cornoid lamella is difficult to recognize. There are various forms, which may present in an isolated or combined way, but terminology and classification are still a matter of discussion.1–3
In the classical variant described by Mibelli, patients develop one or several plaquelike lesions on the extremities (Fig. 3.146). It usually presents in adulthood as persistent lesions that are highly resistant to therapy.6
Eruptive pruritic papular porokeratosis is an intensely itchy eruptive variant of disseminated porokeratosis that can be easily misdiagnosed as prurigo nodularis.16,17
In follicular porokeratosis the cornoid lamella is limited to the follicular ostia. Persistent follicle-centered aggregated papules or erythematous or brown-colored annular plaques with a peripheral keratotic ridge develop on the trunk, limbs, genitogluteal area, and face.18
Porokeratosis ptychotropica (from the Greek ‘ptyche’: fold) presents with symmetrical brownish to reddish macules or plaques distributed on the buttocks, natal cleft, and scrotum (Fig. 3.149).19 The typical presence of multiple cornoid lamellae as seen histologically (punctate type of porokeratosis) explains the clinical keratotic or verrucous appearance and expansile papular growth of the lesions. This highly pruritic disease is mostly confined to men ranging from 6 to 84 years of age.20,21
Giant porokeratosis presents with large lesions that may grow up to 20 cm in diameter with a surrounding elevated edge of 1 cm. This rare form is most often seen on the foot. Large lesions are said to have the highest potential for malignant transformation.7,8
Disseminated superficial actinic porokeratosis (DSAP), the most common variant, is characterized by numerous small, dry, shallow lesions arising on sun-damaged skin of adults (Fig. 3.147).9 It may also complicate PUVA therapy and develop in the immunocompromised. Presentation is in the third and fourth decades and despite its relationship to sunlight, rarely affects the face. The legs, forearms, back, upper arms, and thighs are most commonly affected, in decreasing order of frequency.10
Disseminated superficial (nonactinic) porokeratosis is clinically similar to DSAP, except for a younger age of onset and involvement of both sun-protected and sun-exposed areas.3
In porokeratosis palmoplantaris et disseminate palms and soles are initially affected, but any site, including mucous membranes, may be involved.
Reticular erythema with ostial porokeratosis a rare form of punctate porokeratosis typically missing the classic marginated rim. It is characterized by reticular erythema associated myriad papules developing in a symmetric distribution on the inner aspects of arms and legs. Histology shows cornoid lamellae within the appendageal ostia.22
Porokeratoma is a tumorlike hyperkeratotic nodule or plaque lacking any keratotic rim, preferentially on the distal limbs. Histology reveals an area of well demarcated verrucous epidermal hyperplasia with multiple broad cornoid lamellae. Since other manifestations of porokeratosis are missing the relationship to porokeratosis is contentious. An incidental formation of a cornoid lamella in an acanthoma of any kind may occasionally be seen.23
CAP syndrome is a rare autosomal recessive disorder featuring craniosynostosis, genitourinary and anal anomalies and porokeratosis-like lesions.24,25
112 Disorders of keratinization
A
B
Porokeratosis has an increased risk of developing Bowen disease, and basal cell and squamous cell carcinoma.26–32 The reported incidence varies from 6.8% to 11.6% and depends on size, duration, age of the patient, immune status, treatment with radiotherapy and the type of porokeratosis.30,31 Tumors usually develop many years after the onset of the disease, are frequently multiple, and arise most often on large or coalescing lesions on the trunk and extremities, particularly in porokeratosis linearis and DSAP.33
Pathogenesis The presence of localized dysplastic features indicates a focal, expanding clone of abnormal keratinocytes associated with the development of a cornoid lamella.34 Porokeratotic lesions have been shown to be associated with abnormal epidermal DNA ploidy in association with increased DNA indices, midway between normal skin and Bowen disease.35,36 Chromosomal abnormalities have been identified within cultured keratinocytes and fibroblasts derived from patients suffering from both the localized and Mibelli variants of the disease.37,38 The mutations found in the short arm of chromosome 3 may be associated with a wide variety of malignancies.39 Ionizing radiation, ultraviolet light, including sun tanning beds, and PUVA may be
associated with the development of new skin lesions in porokeratosis.40 The first may be of particular relevance in the development of malignancy in these lesions.41
Proteins p53 and pRb are overexpressed within keratinocytes immediately beneath and adjacent to the cornoid lamellae; mdm-2 and p21waf-1 are reduced.42–45 This imbalance in cell cycle control mechanisms offers a potential explanation for the development of malignancy in porokeratosis although to date p53 mutations have not been identified.44,46 The possibility of an infective etiology remains.47 Some evidence of HPV infection in two patients with porokeratosis of Mibelli has been reported.48
113 Acquired palmoplantar keratoderma and malignancies
There are associations of porokeratosis with autoimmune and other diseases (systemic lupus erythematodes, dermatomyositis, psoriasis, vitiligo, alopecia areata, lichen planus, lichen sclerosus et atrophicus, pemphigus, diabetes, rheumatoid arthritis, Crohn disease, liver or renal dysfunction, pancreatitis, and others), neoplasms (hepatocellular-, cholangiocarcinoma, hereditary non-polyposis colorectal carcinoma, lymphoma, leukemia, myeloma, mycosis fungoides, and others), and genetic disorders (Werner syndrome, Rothmund-Thomson syndrome, cystic fibrosis, trisomy 16, erythropoietic protoporphyria, and pseudoxanthoma elasticum).1,2
DSAP has been mapped in Chinese pedigrees to chromosomes 12q, 15q,18p and 16q.49–52 More recently, heterozygous mutations in the MVK gene have been reported in porokeratosis of Mibelli and in DSAP.53–56 MVK encodes mevalonate kinase which is involved in regulation of keratinocyte differentiation and protection of keratinocytes from UVA-induced apoptosis.53 For DSAP, candidate genes include SART3 involved in regulation of messenger RNA splicing, SSH1, and ARPC3 which play a role in polymerization and dynamics of actin filaments.2 In porokeratosis Mibelli overexpression of EMILIN2, a pro-apoptotic gene may cause abnormal apoptosis of epidermal keratinocytes and alter the process of keratinization.57
Trigger and risk factors for porokeratosis, in particular porokeratosis of Mibelli, disseminated superficial actinic and nonactinic porokeratosis, and eruptive pruritic papular porokeratosis are UV-light, radiation therapy, chronic GVHD, immunosuppression (iatrogen, AIDS, hereditary deficiencies), infections (HPV, HIV, HCV, HSV), drugs (furosemide, antibiotics, TNFα inhibitor, hydroxyurea, systemic and topical steroids, immunosuppressive agents, and others). Local factors reported are lymphedema and scar formation following burns or access regions of hemodialysis.16,17,58–62
Histologic features The biopsy must be taken through the peripheral grooved ridge. If the long axis of the specimen does not transact the border, the diagnostic features will be missed.63 Typical changes consist of a keratin-filled epidermal invagination with an angulated parakeratotic tier, the cornoid lamella (Fig. 3.150). Drawing a line perpendicular to the cornoid lamella on the surface of a punch immediately after the biopsy has been taken and before fixation, guarantees proper orientation when the specimen is bisected in the laboratory.63 The corneocytes of the cornoid lamella express characteristic PAS-positive granules.64 Formation of a cornoid lamella can also be seen in hair follicles or acrosyringia (Fig. 3.151). The involvement of the sweat pores explains the original term ‘poro’-keratosis. The keratinocytes below the cornoid lamella are large, vacuolated, and pleomorphic and do not form a granular layer. Dyskeratotic cells may be present and epithelial dysplasia, ranging from mild changes through to carcinoma in situ, may occasionally be seen. Beneath, a variably dense lichenoid lymphocytic infiltrate, sometimes with features of interface dermatitis or subepidermal clefting, colloid bodies and amyloid material, is sometimes seen.65,66 The adjacent epithelium
A
B
C
114 Disorders of keratinization
A
towards the center of the lesion is often atrophic, but may be of normal thickness or even acanthotic with extensive hyperkeratosis (Fig. 3.152). The papillary dermis below is thickened and sometimes shows a lymphocytic infiltrate, melanophages, telangiectatic vessels, fibrosis, and loss of elastic fibers.66,67 The typical features are best identified in the Mibelli variant. Changes tend to be less pronounced in the other subtypes. In the actinic variant there is often solar elastosis and atrophy of the adjacent epidermis. The pigmented variant of porokeratosis reveals melanocyte hyperplasia and pigment incontinence, which explains why it clinically mimics a melanocytic lesion.68 In punctate types of porokeratosis there is no elevated keratotic rim but multiple focal or reticulated parkeratotic tiers above epidermal invaginations (Fig. 3.153).3,19
B
Differential diagnosis PAON is a verrucous nevus due to germline mutations of connexin 26 and it is not related to porokeratosis. Histology shows an ortho- or parakeratotic filiform keratosis protruding from the dilated ostia of eccrine acrosyringia or hair follicles. PAON also features vacuolated and pyknotic keratinocytes, but lacks dyskeratosis, pleomorphism, and interface dermatitis as found in porokeratosis.69,70
Signs of interface dermatitis and regression may lead to the misdiagnosis of benign lichenoid keratosis when the cornoid lamella is not seen in the initial sections, therefore further deeper sections are helpful in reaching a diagnosis.71,72
Cornoid lamella formation, however, does occur as a non-specific, incidental finding in a variety of conditions, including psoriasis vulgaris, dermatomyositis (Wong-type), Grover disease, HIV-associated epidermodysplasia verruciformis, keratosis lichenoides chronica (Nekam disease), seborrheic keratosis, solar keratosis, verruca vulgaris, and squamous cell and basal cell carcinomas.3,73 Cornoid lamellae are also seen in inflamed linear verrucous epidermal nevus (ILVEN), ichthyosis hystrix Curth-Macklin, and PC. They are also not uncommon in normal, and particularly actinically damaged skin.1,3 These non-porokeratotic conditions do not feature large, vacuolated, pleomorphic or dyskeratotic keratinocytes below the cornoid lamella.
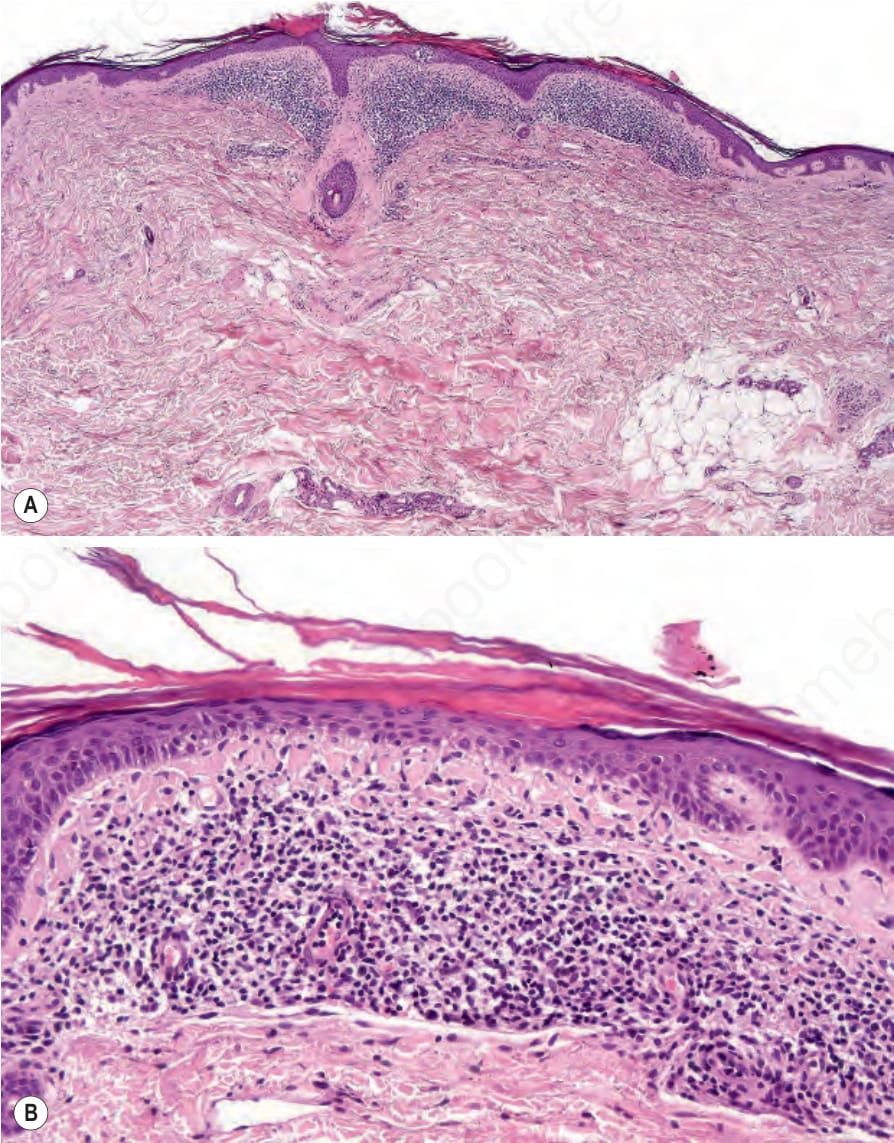
Fig. 3.145 Flegel disease: (A) scanning view of an established lesion showing focal hyperkeratosis, and a superficial bandlike infiltrate; (B) there is hyperkeratosis, focal epidermal atrophy, vacuolization of the dermal–epidermal junction with many colloid bodies, below a dense lymphocytic infiltrate.
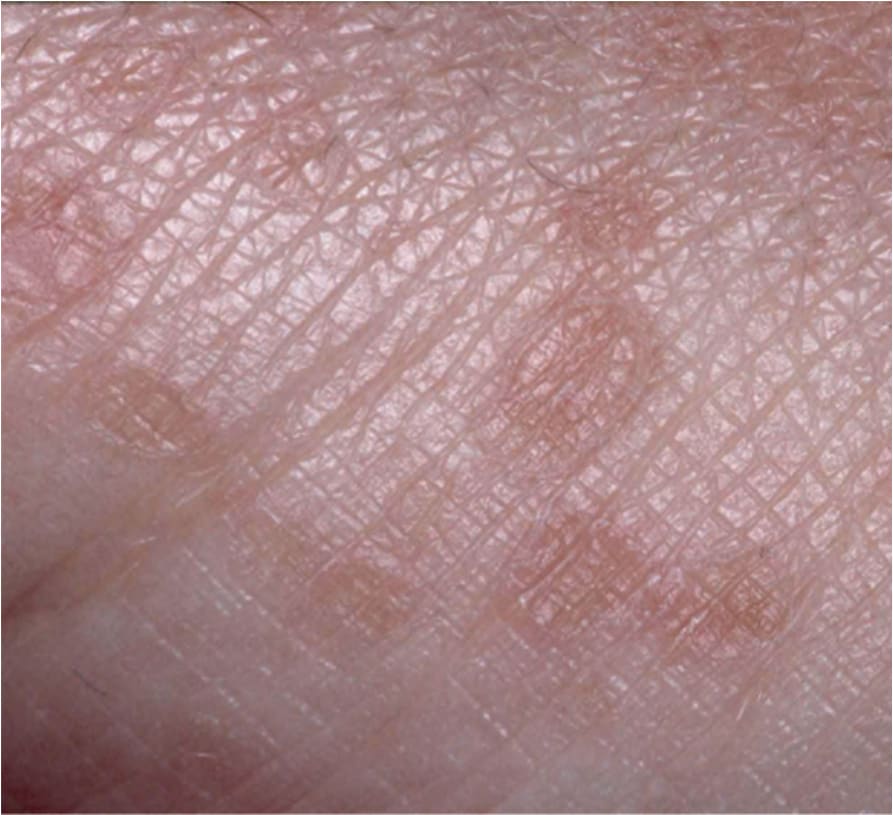
Fig. 3.146 Porokeratosis of Mibelli: the lesions are erythematous, atrophic and scaly, with a sharply defined and slightly raised keratotic rim.
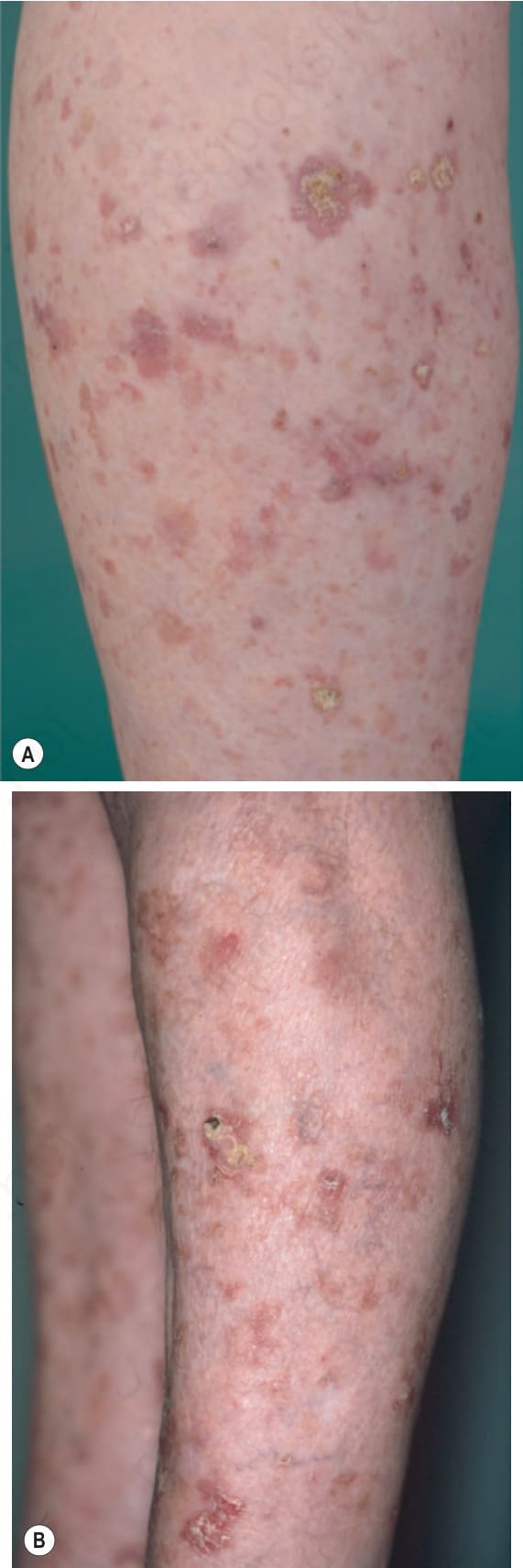
Fig. 3.147 Disseminated superficial actinic porokeratosis: (A) there are numerous small, reddish or brownish keratotic macules on sun damaged skin; (B) squamous cell carcinoma developed in the crusted and hyperkeratotic lesion.

Fig. 3.148 Linear porokeratosis: in this variant, the lesions have a half-sided linear and reticulated nevoid distribution.

Fig. 3.149 Porokeratosis ptychotropica: brownish to reddish macules or plaques appear symmetrically distributed on the buttocks and natal cleft.
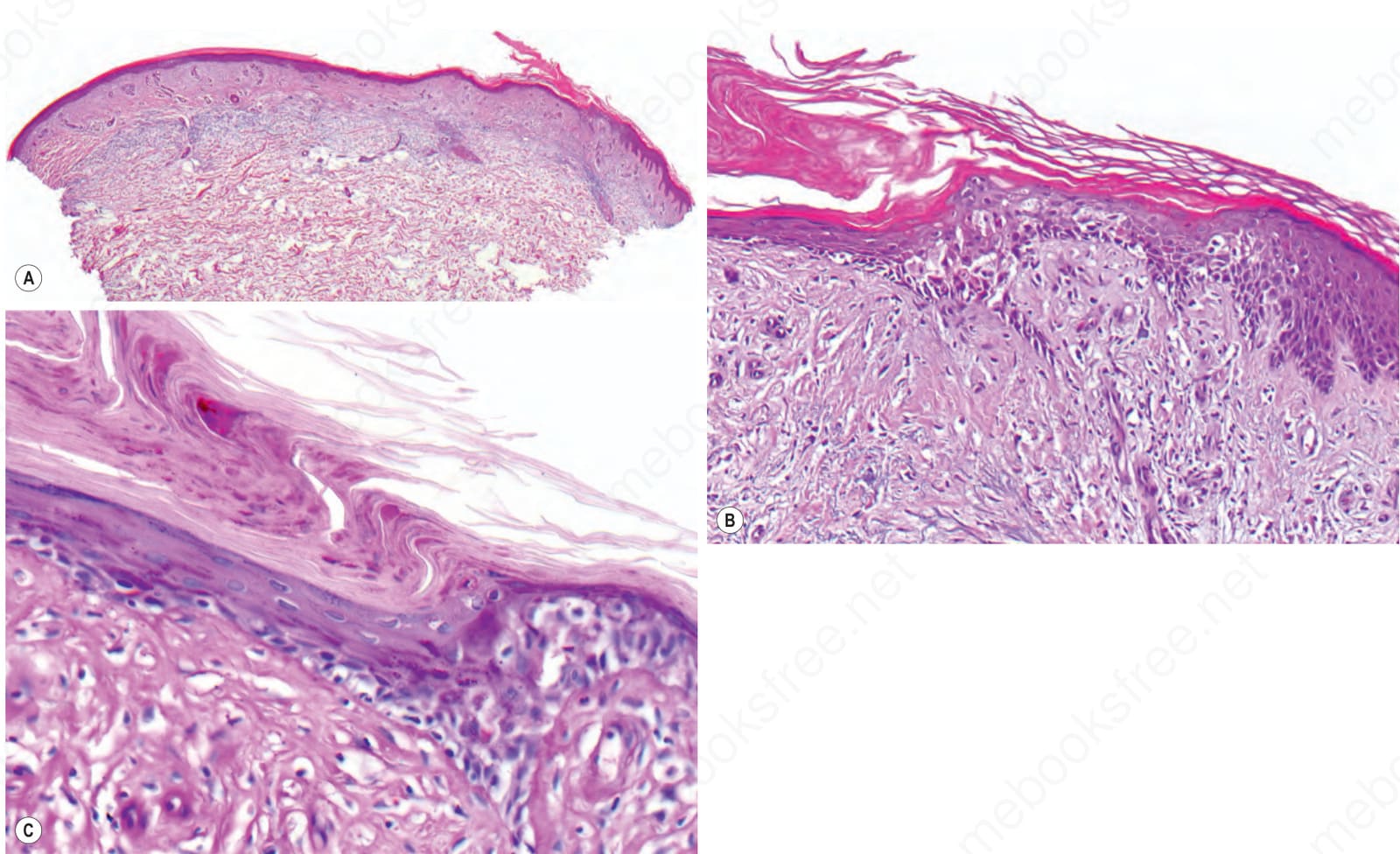
Fig. 3.150 Porokeratosis of Mibelli: (A) on the right side the diagnostic features is a keratin-filled epidermal invagination with an angulated keratotic tier, the cornoid lamella. The center of the lesion is atrophic. (B) The epidermis below the cornoid lamella expresses large, vacuolated, and pleomorphic keratinocytes and does not form a granular layer. (C) The corneocytes of the cornoid lamella are parakeratotic and express characteristic PAS-positive granules.
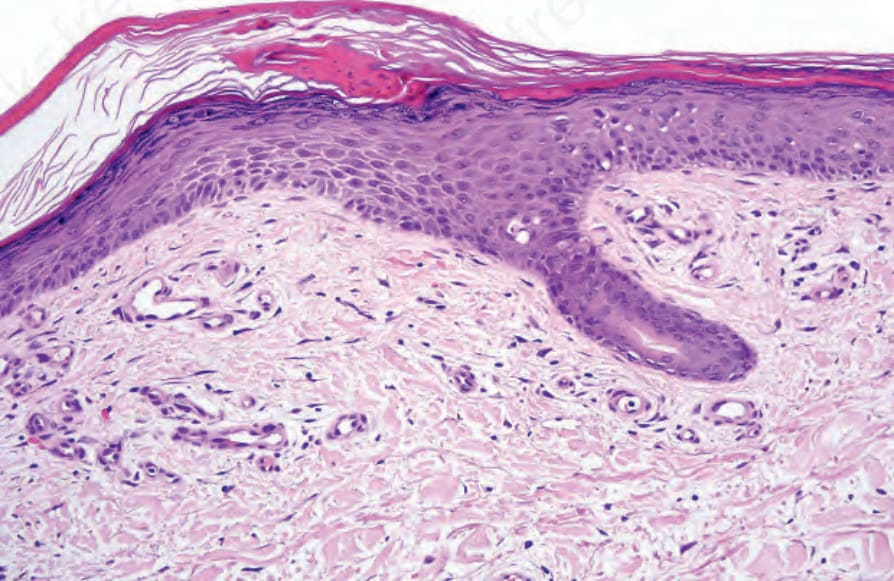
Fig. 3.151 Disseminated superficial actinic porokeratosis: in this example, the cornoid lamella has arisen overlying an acrosyringium. The epidermis towards the center of the lesion appears atrophic and the papillary dermis contains ectatic blood vessels.
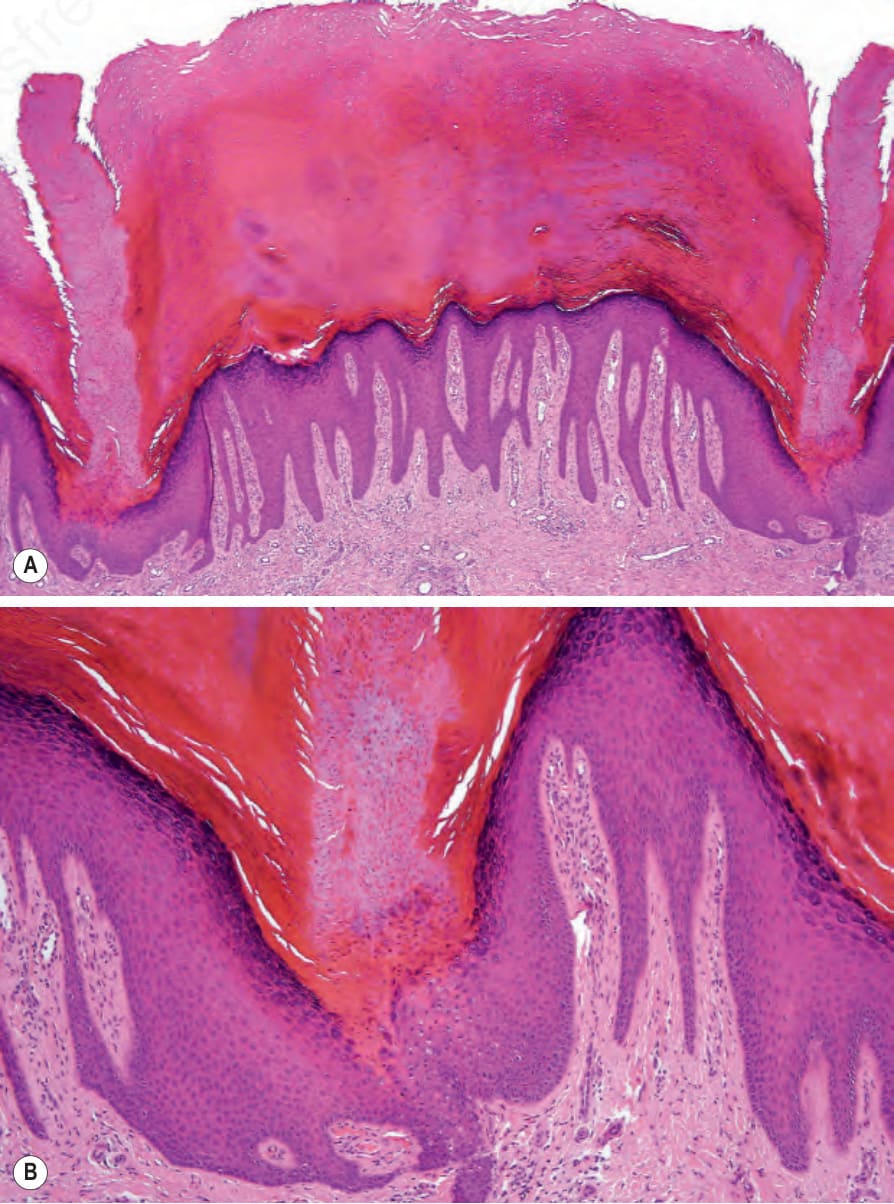
Fig. 3.152 Porokeratosis of Mibelli: (A) there is central orthohyperkeratosis with two welldeveloped cornoid lamellae on both sides. Note the epidermal depression at their bases. (B) The cornoid lamella can be seen to be composed of a column of parakeratosis.
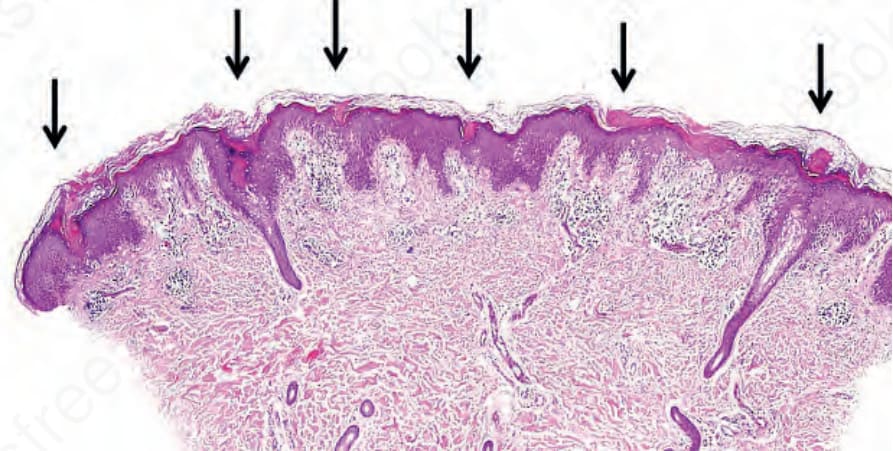
Fig. 3.153 Porokeratosis ptychotropica: there is no solitary keratotic rim on the lateral side but multiple parakeratotic tiers above epidermal invaginations (arrows), a characteristic feature of the punctate type of porokeratosis.