Flegel disease (hyperkeratosis lenticularis perstans)
Flegel disease (hyperkeratosis lenticularis perstans)
Clinical features Flegel disease (hyperkeratosis lenticularis perstans) is a rare autosomal dominant disorder of cornification presenting in older individuals, usually between the third and fourth decades of life.1,2 A large number of discrete red-brown scaly papules with discrete irregular margins (‘cornflake sign’) develop over the dorsa of the feet and on the lower parts of the legs (Fig. 3.144). The lesions may spread to the upper part of the legs and thighs, more rarely over the arms and trunk or concha of the ear.3–5 On palms and soles punctate keratoses have been described.6 The lesions are either asymptomatic or mildly pruritic. Characteristically, removal of the scale is associated with pinpoint bleeding, a feature that distinguishes this disorder from stucco keratoses. Other than an isolated report of an increased incidence of both basal cell and squamous carcinoma, there is no particular associated risk of malignancy.7
B
Pathogenesis and histologic features The causative mutation remains unknown. A low proliferation rate of keratinocytes together with downregulation of filaggrin, loricrin, and high molecular weight keratins, and loss of the keratin pattern in the horny layer, suggests a retention hyperkeratosis and complex dysregulation of epidermal differentiation.8,9
Histologically, there is hyperkeratosis with a focal parakeratosis overlying a thinned, flat epidermis with loss of keratohyalin granules. In the periphery of the lesions the epidermis is acanthotic with collarette-like elongated rete ridges. A lymphocytic lichenoid infiltrate with colloid body formation is displayed in early lesions (Fig. 3.145).10 The lymphocytes are an
admixture of CD4+ T-helper cells and, less frequently CD8+ T-cytotoxic/ suppressor cells. Sézary-like cells have been described. Langerhans cells are highly reduced.8
Ultrastructural features consist of rudimentary keratohyalin granules, absence of, vacuolation of or abnormally lamellated membrane coating (Odland) bodies, failure to form compact keratin, and also to form a cornified envelope in the corneocytes.9,11

Fig. 3.144 Flegel disease: (A) there are characteristic disseminated erythematous scaly lesions; (B) the lower legs are commonly affected. Lesions are small, multiple and show irregular margins covered by a well-developed scale (‘cornflake sign’). By courtesy of M. Price, MD, Institute of Dermatology, London, UK.
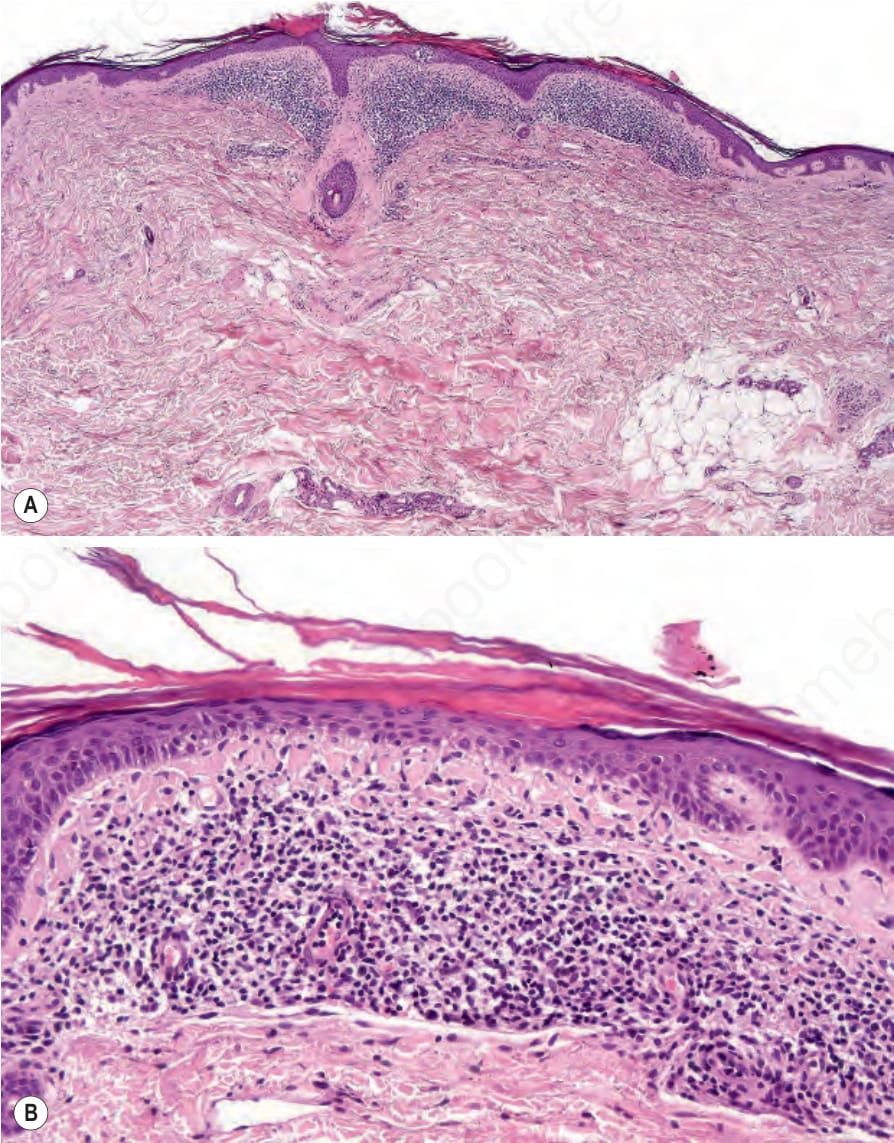
Fig. 3.145 Flegel disease: (A) scanning view of an established lesion showing focal hyperkeratosis, and a superficial bandlike infiltrate; (B) there is hyperkeratosis, focal epidermal atrophy, vacuolization of the dermal–epidermal junction with many colloid bodies, below a dense lymphocytic infiltrate.