Keratolytic winter erythema
Keratolytic winter erythema
Clinical features Keratolytic winter erythema (synonyms: erythrokeratolysis hiemalis, Oudtshoorn disease) is an autosomal dominant disorder first described in South Africa.1 Sporadic cases have been reported from other countries.2,3 The
108 Disorders of keratinization
region containing an active enhancer element for CTSB, resulting in upregulation of this gene in affected individuals, have been found.8
Biopsy of the advancing edge of a lesion shows hyperplasia, spongiosis, and, in the upper stratum spinosum, keratinocytes with pale cytoplasm, perinuclear vacuolization, and pyknotic nuclei. In the absence of a granular layer the epidermis forms a parakeratotic wedge, which becomes sandwiched within the hyperkeratotic stratum corneum and is eventually shed (Fig. 3.139).1 During regeneration undifferentiated keratinocytes are not confined to the basal layer but appear in the lower half of the epidermis.1 A superficial perivascular lymphocytic infiltrate has been reported by some authors.3
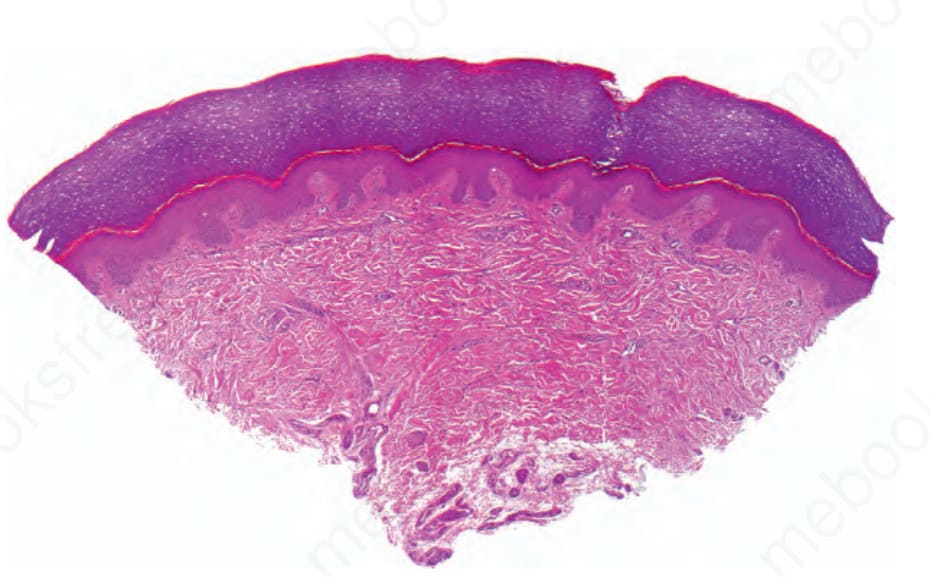
Fig. 3.136 Transient aquagenic keratoderma: note the wide opening of an acrosyringeal ostium, and the pale staining of an orthohyperkeratotic stratum corneum, otherwise there are no other histologic changes.
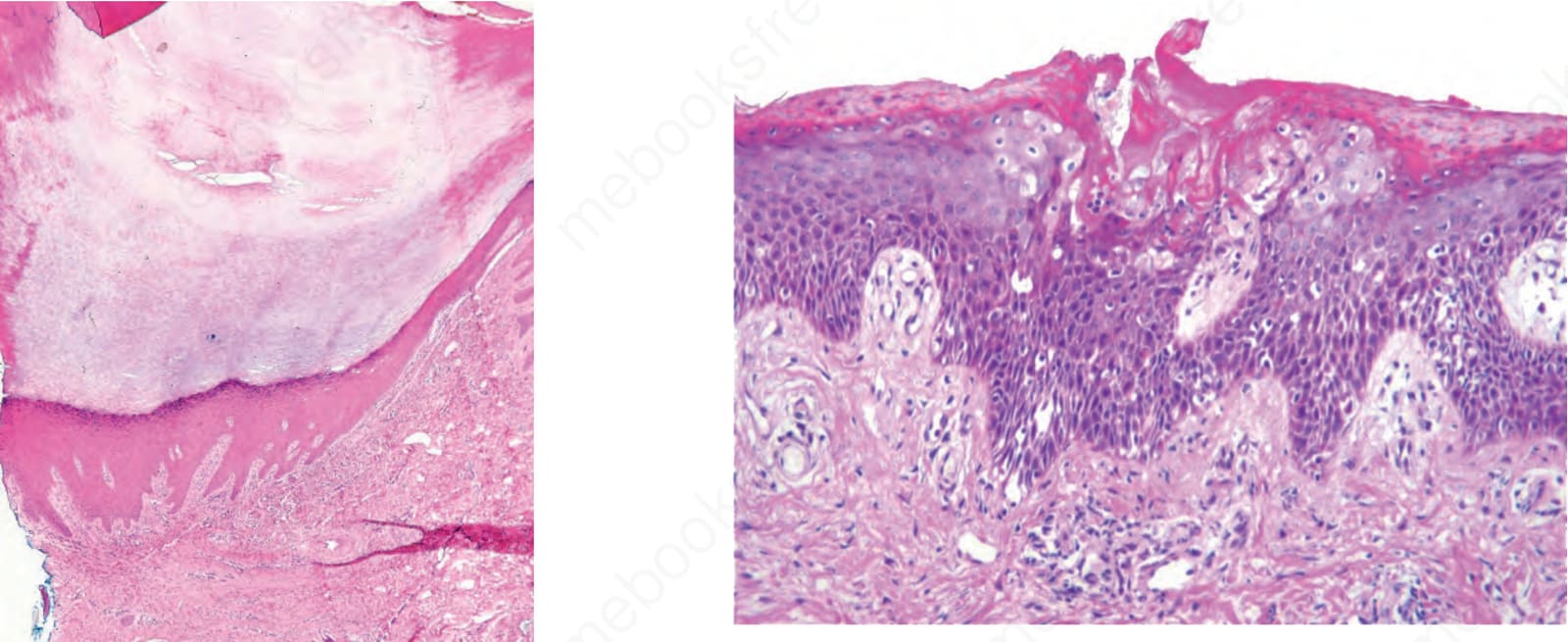
Fig. 3.139 Keratolytic winter erythema: there is hyperplasia and spongiosis of the epidermis. The stratum granulosum is absent. Keratinocytes show a pale cytoplasm, perinuclear vacuoles, and pyknotic nuclei. A parakeratotic wedge is seen within the hyperkeratotic stratum corneum. By courtesy of W. Grayson, MD, University of the Witwatersrand, Johannesburg, South Africa.