Howel-Evans syndrome
Howel-Evans syndrome
Clinical features Howel-Evans syndrome (tylosis with esophageal carcinoma) is a syndromic autosomal dominant palmoplantar keratoderma that develops by 6 to 15 years of age and is associated with high risk of esophageal carcinoma.1 Affected individuals develop painful hyperkeratoses on the pressure areas of the balls of the feet, with milder involvement of the palms, which disappear with prolonged bed rest (Fig. 3.109).1–5 In contrast to pachyonychia nails are unaffected.6 Other features are oral leukokeratosis, keratosis pilaris, dry rough skin, and multiple epithelial cysts. The oral leukokeratosis typically predates the onset of keratoderma and is an important diagnostic clue of early involvement in family members.5–9 In the largest kindred reported to date, 28% developed esophageal squamous carcinoma of whom 84% died of their tumor.4
Pathogenesis and histologic features This condition is caused by mutations in the WNT10A gene encoding a signaling molecule that is essential for the development of ectodermal appendages.6 Phenotypic heterogeneity is the rule with mutations in WNT10A causing disorders ranging from monosymptomatic severe oligodontia to Schöpf-Schulz-Passarge syndrome.7
Multiple eccrine syringofibroadenomas and squamous cell carcinomas may arise on the acral surfaces in older patients. The eyelid lesions represent apocrine hidrocystomas (Fig. 3.112).1,3,5
97 Palmoplantar keratoderma
A
B
on soles over pressure points (Fig. 3.113). Lesions evolve in adolescence or early adulthood and are exacerbated by mechanical stress. Pain and hyperhidrosis may accompany the keratoderma.6
Pathogenesis and histologic features The most frequent form, SPPK type 1 is caused by mutations in DSG1 encoding desmoglein 1. However, mutations in DSG1 may also result in a diffuse form of PPK.7,8 Interestingly, carriers of heterozygous mutations in DSG1 develop striate PPK only while the offspring of two such heterozygous carriers can suffer from the SAM syndrome (severe dermatitis-multiple allergies-metabolic wasting syndrome).9 SPPK type 2 is due to mutations in the desmoplakin gene (DSP).10 In SPPK type 3 a frameshift mutation in the V2 tail domain of keratin 1 has been identified.11 The mutation is similar to those being reported in ichthyosis Curth-Macklin.12

Fig. 3.109 Howel-Evans syndrome: (A) focal autosomal dominant palmoplantar keratoderma is associated with an increased risk of esophageal squamous carcinoma; (B) in this patient, the palms were also severely affected. By courtesy of the Institute of Dermatology, London, UK.

Fig. 3.110 Schöpf-Schulz-Passarge syndrome: diffuse keratoderma on palms and fingers is associated with nail dystrophy.
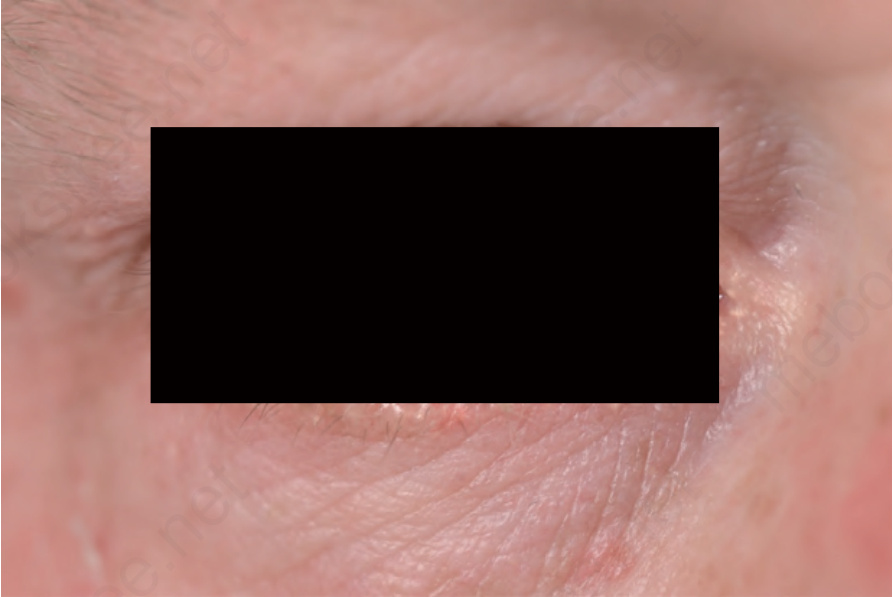
Fig. 3.111 Schöpf-Schulz-Passarge syndrome: multiple yellowish and bluish cysts on the eyelids.
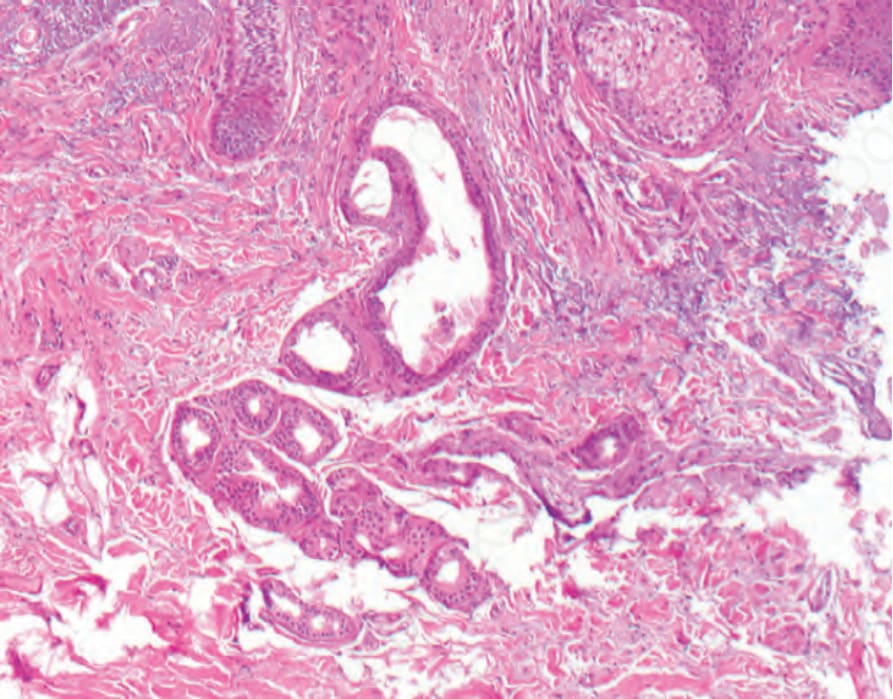
Fig. 3.112 Schöpf-Schulz-Passarge syndrome: the cysts on the eyelids represent apocrine hidrocystomas.

Fig. 3.113 Striate palmoplantar keratoderma: (A) linear hyperkeratotic bands along the palms and flexural side of the fingers; (B) island-like areas of hyperkeratosis on the soles over pressure points.