Papillon-Lefèvre syndrome
Papillon-Lefèvre syndrome
Clinical features Papillon-Lefèvre syndrome (palmoplantar keratoderma with periodontopathia) is characterized by a diffuse, transgradient keratoderma and redness of the palms and soles (Fig. 3.105).1 Pseudoainhum and hyperkeratotic lesions on elbows and knees can occur (Fig. 3.106). Additional features are periodontitis in childhood and premature loss of teeth (Fig. 3.107).2–9 There is a predisposition to furunculosis, cerebral and liver abscesses, and other pyogenic infections.8–10 Retinoid therapy not only improves the hykeratoses, but also diminishes oral and infectious complications.11,12 There is a risk for development of melanoma and/or squamous cell carcinoma.13–15 Haim-Munk syndrome is allelic with Papillon-Lefèvre syndrome and
Pathogenesis and histologic features Papillon-Lefèvre syndrome has an autosomal recessive mode of inheritance and is associated with missense and nonsense mutations, deletions, and insertions in the gene for the lysosomal cysteine protease cathepsin C (dipeptidyl aminopeptidase I).18–22 In homozygous patients, loss of cathepsin C activity results in impaired activation of bone marrow myeloid and macrophage granule serine proteases with resultant defective bacterial phagocytosis.23–28 The cathepsin C gene is also expressed in squamous epithelium of the palms, soles, knees, and the oral keratinized gingiva.19
The histopathological features of the palmoplantar lesions show marked hyperkeratosis with acanthosis and a thickened granular cell layer (Fig. 3.108). Parakeratosis and epidermal psoriasiform hyperplasia have also been described. The elbow and knee lesions show epidermal psoriasiform hyperplasia with parakeratosis, elongation of the dermal papillae, and dilatation of the superficial dermal vasculature.
96 Disorders of keratinization
Pathogenesis and histologic features Missense mutations in RHBDF2 (rhomboid 5 homolog 2) encoding an intramembrane protease have been identified.10–13 Functional data suggest that mutant RHBDF2 increases signaling through the epidermal growth factor receptor (EGFR), which promotes hyperproliferation, dysregulation of wound repair and as such predisposes to precancerous lesions.13
The cutaneous lesions are characterized by hyperkeratosis, hypergranulosis, and acanthosis. Features of epidermolytic hyperkeratosis are absent.
The buccal mucosal lesions are characterized by parakeratosis, acanthosis, and spongiosis accompanied by cytoplasmic vacuolation of the prickle cell layer.4

Fig. 3.105 Papillon-Lefèvre syndrome: (A) there is marked hyperkeratosis affecting the soles of the feet; (B) in this patient, the dorsal aspects of the hands, particularly the knuckles are also affected. By courtesy of W.A.D. Griffiths, MD, Institute of Dermatology, London, UK.

Fig. 3.106 Papillon-Lefèvre syndrome: a scaly psoriasiform plaque is present over the elbow. By courtesy of W.A.D. Griffiths, MD, Institute of Dermatology, London, UK.

Fig. 3.107 Papillon-Lefèvre syndrome: gingival inflammation and swelling with the characteristic irregular positioning of the teeth which, as a result of destruction of supporting tissues, have shifted under the forces of mastication. This patient is a 12-year-old child, but the severity of the periodontal destruction is what might be expected in a person aged 60 years. By courtesy of R.A. Cawson, MD, Guy’s Hospital, London, UK.
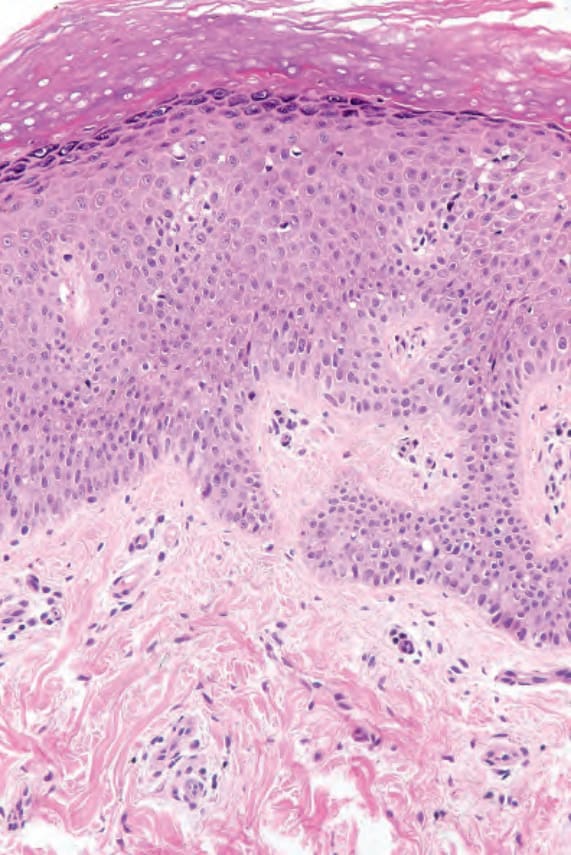
Fig. 3.108 Papillon-Lefèvre syndrome: there is hyperkeratosis, hypergranulosis and acanthosis.