Loricrin keratoderma
Loricrin keratoderma
Clinical features
Loricrin keratoderma (Camisa variant of Vohwinkel syndrome, Vohwinkel keratoderma with ichthyosis) is inherited in an autosomal dominant fashion and characterized by a diffuse palmoplantar keratoderma that is very similar to that of Vohwinkel syndrome, including the honeycomb-like appearance (Fig. 3.98).1–3 In contrast to true Vohwinkel syndrome the edges of the keratoderma are diffuse, cicatricial bands (pseudo-ainhum) are less mutilating, and warty papules and starfish-like keratosis are not a prominent feature. A concomitant ichthyosis with generalized fine scaling is a constant feature and often presents congenitally prior to the development of
93 Palmoplantar keratoderma
A
B
Histologic features of loricrin keratoderma consist of psoriasiform hyperplasia of the epidermis, hyperkeratosis with small roundish nuclear debris in the upper horny layer and focally, expression of transitional cells, i.e., parakeratotic cells with prominent oval nuclei above the granular layer. The stratum granulosum is prominent and perinuclear vacuolization is sometimes seen (Figs 3.99 and 3.100). Inflammation is almost absent.6 The nuclei of keratinocytes demonstrate a characteristic immunoreactivity for loricrin that is not seen in any other type of PPK.10
the palmoplantar keratoderma.2 Patients do not suffer from deafness as seen in Vohwinkel keratoderma.
Pathogenesis and histologic features Mutations on chromosome 1q21 that result in aberrant, elongated C-terminal domains of one loricrin allele may lead to abnormal loricrin expression, and impairment of cross-linking within the protein and with other cornified envelope proteins.3–6 Mutant loricrin is segregated into the nucleus where is thought to impair the function of profilaggrin to mediate nuclear dissolution in the course of apoptosis which represents an integral part of keratinocyte terminal differentiation.7,8 Loricrin keratoderma, and some cases of progressive symmetrical erythrokeratoderma, may share the mutation and light microscopy and ultrastructural features.7 Therefore some authors have proposed that loricrin keratoderma should include cases of what has been formerly termed either (Vohwinkel) keratoderma with ichthyosis or progressive symmetrical erythrokeratoderma.9
Electron microscopy characteristically reveals formation of a well-formed transitional layer, intranuclear granules in the upper stratum granulosum, and a thin cornified envelope.7
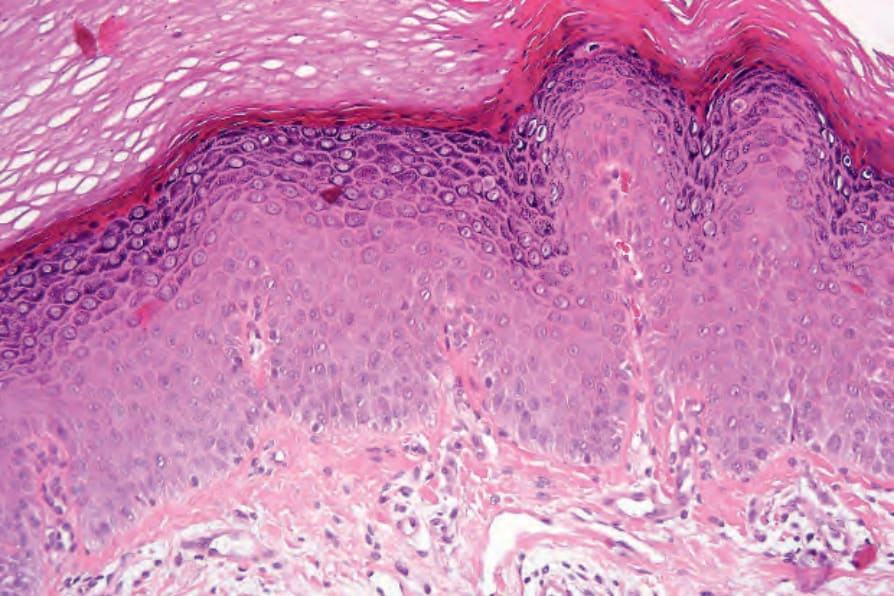
Fig. 3.100 Loricrin keratoderma: the stratum granulosum is prominent and scattered cells (on the right side of the field) show perinuclear vacuolization. The parakeratotic keratinocytes in the lower horny layer represent transitional cells. In the upper horny layers small roundish residual nuclei are preserved.

Fig. 3.98 Loricrin keratoderma: (A) there is a generalized fine scaling; (B) palmoplantar keratoderma with a yellowish papular and honeycomb-like appearance but less mutilating than in classical Vohwinkel syndrome.
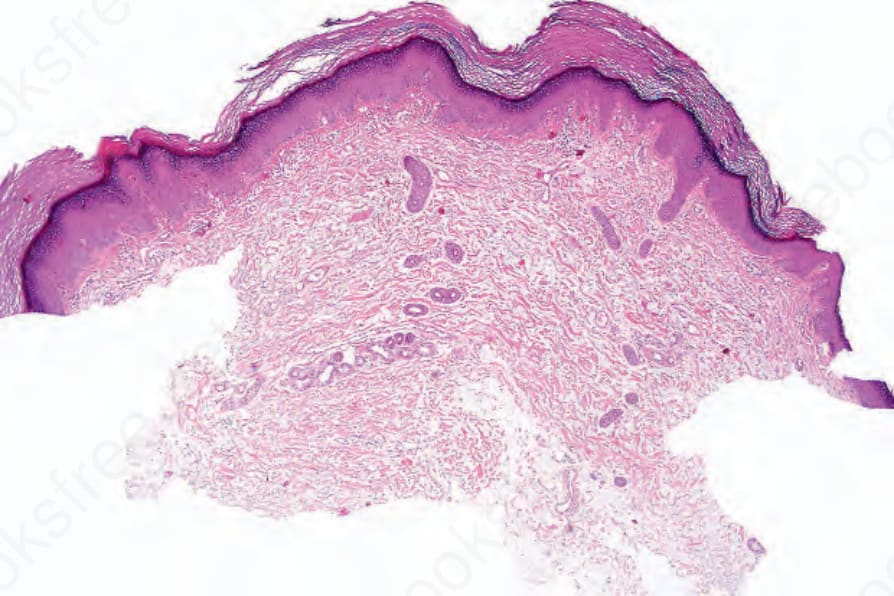
Fig. 3.99 Loricrin keratoderma: there is hyperkeratosis and mild acanthosis.