Huriez syndrome
Huriez syndrome
Clinical features In Huriez syndrome (keratosis palmoplantaris diffusa with sclerodactyly and sclerothylosis) patients present with diffuse mild palmoplantar keratoderma, scleroatrophic skin of the limbs, hypoplasia and dystrophy of the nails, and
hypohidrosis (Fig. 3.94).1–3 Aggressive squamous cell carcinoma develops in the affected skin in approximately 15% of the cases. It has an early onset with a high risk of metastasis in the third to fourth decades.4 Huriez syndrome shares some features with a complex syndrome defined by diffuse palmoplantar hyperkeratosis with squamous cell carcinoma and sex reversal.7–9
Pathogenesis and histologic features The gene responsible for Huriez syndrome has been mapped to 4q23.5 Histology shows mild acanthosis, orthohyperkeratosis, and well developed
91 Palmoplantar keratoderma
A
granular layer (Fig. 3.95). Interestingly, immunohistochemical and ultrastructural studies reveal an absence of Langerhans cells in involved skin.4,6
B
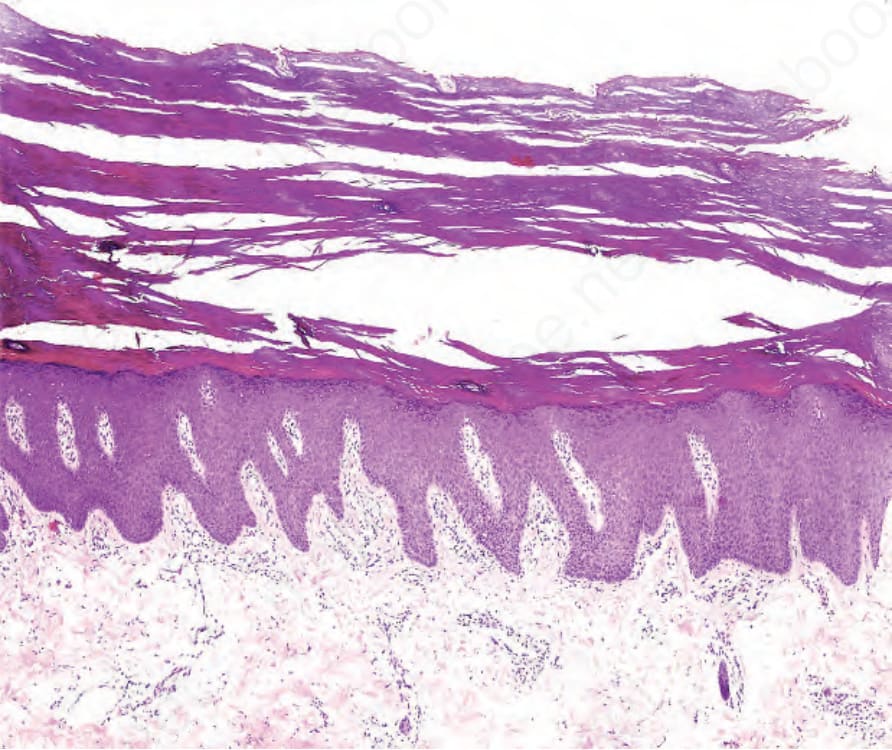
Fig. 3.90 Mal de Meleda: there is orthohyperkeratosis, hypergranulosis, and prominent papillomatosis, the latter feature is characteristic for Mal de Meleda.
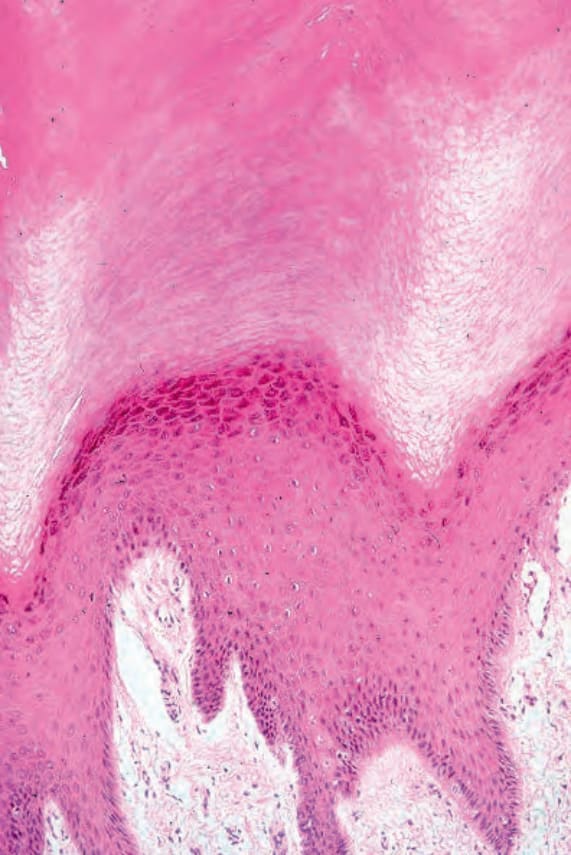
Fig. 3.91 Diffuse non-epidermolytic palmoplantar keratoderma: there is massive hyperkeratosis, hypergranulosis, and acanthosis. Absence of epidermolytic hyperkeratosis rules out diffuse palmoplantar keratoderma Vörner-Unna-Thost.

Fig. 3.94 Huriez syndrome: (A) the main features are sclerodactyly, hypotrophic and dystrophic nails; (B) there is diffuse, mild palmar keratosis.
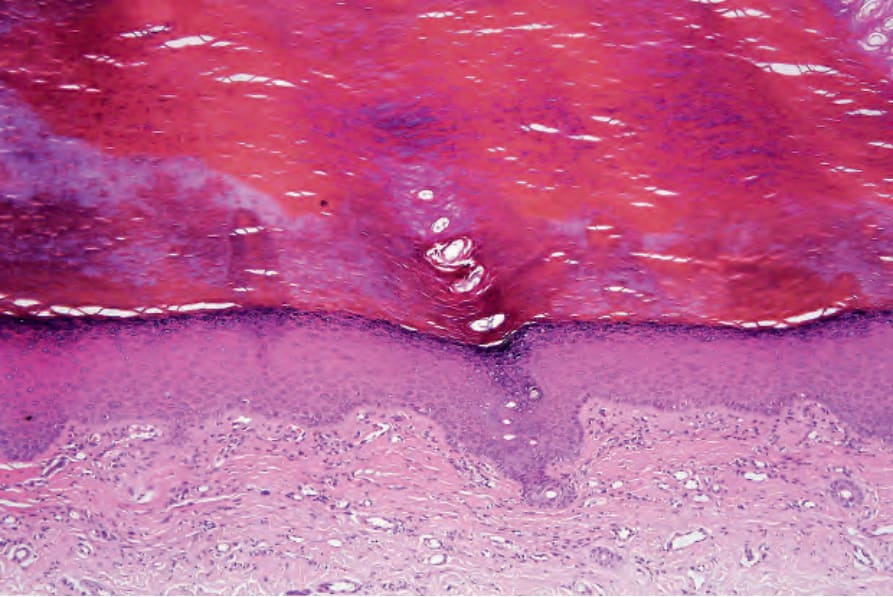
Fig. 3.95 Huriez syndrome: there is mild acanthosis, orthohyperkeratosis and a welldeveloped granular cell layer.