Epidermolytic palmoplantar keratoderma
Epidermolytic palmoplantar keratoderma
Clinical features Epidermolytic palmoplantar keratoderma (syn. keratosis palmoplantaris diffusa Vörner-Unna-Thost) represents the most common form of palmoplantar keratoderma with an incidence of 1 : 100 000. Reinvestigation of the original family with Unna-Thost PPK showed that epidermolytic forms existed within the family as had been described by Vörner. Therefore, it is not justified to separate Vörner disease from Unna-Thost disease. The unifying designation epidermolytic palmoplantar keratoderma seems more appropriate.1,2
This nonsyndromic PPK is inherited as an autosomal dominant and usually presents in the first years of life when the patients start running.1–7
87 Palmoplantar keratoderma
Palmoplantar keratoderma Disease Inheritance Gene (Protein) Symptoms
Diffuse Huriez syndrome AD ? Sclerodactyly, nail dystrophy, squamous cell carcinomas in atrophic areas Vohwinkel syndrome AD GJB2 (Connexin 26) Mutilating keratoderma, sensorineural deafness Loricrin keratoderma AD LOR (Loricrin) Associated ichthyosis KLICK syndrome AR POMP Associated ichthyosis Clouston syndrome AR GJB6 (Connexin 30) Diffuse palmoplantar keratoderma, alopecia, nail dystrophies Olmsted syndrome AD or XR TRPV3 MBTPS2
Diffuse mutilating palmoplantar and periorificial keratoses, ectodermal dysplasia Papillon-Lefèvre syndrome AR CTSC (Cathepsin) Diffuse palmoplantar keratosis with severe periodontitis Naxos syndrome AR or AD JUP (Plakoglobin) Wooly hair, cardiomegaly, tachycardia McGrath syndrome AD PKP1 (Plakophilin 1) Skin fragility, hypotrichosis, hypohidrosis, nail dystrophy, no cardiac complications Schöpf-Schulz-Passarge syndrome
AR WNT10A PPK with eyelid cysts, hypodontia and hypotrichosis
Circumscribed Pachyonychia congenita AD KRT6, KRT16 KRT17
Thickened nails, painful palmoplantar keratoderma, follicular hyperkeratosis, hair abnormalities, cysts, leukokeratosis, natal teeth Howel-Evans syndrome AD RHBDF2 Association with carcinoma of esophagus Richner-Hanhart syndrome AR TAT (Tyrosine amino-transferase) Focal, often painful palmoplantar keratoderma Carvajal-Huerta syndrome AR or AD DSP (Desmoplakin) PPK with dehiscent keratinocytes, wooly hair, arrhythmogenic left cardiomyopathy
Punctate Cole disease AD ENPP1 Punctate keratoderma with guttate hypopigmentation, calcific tendinopathy or calcinosis cutis
Epidermolytic hyperkeratosis Epidermolytic palmoplantar keratoderma Vörner-Unna-Thost, (Greither keratoderma, epidermolytic variant; hereditary painful callosities; PPK nummularis), and others
Patients develop symmetrical, well-demarcated yellowish, smooth and waxy plaques covering the palms and soles, and, to some extent, the ventral surface of fingers and toes (Figs 3.82 and 3.83). The lesions reach the lateral aspects of hands and feet but not beyond. The periphery is bordered by an erythematous margin (Fig. 3.84).3 Painful blisters are not uncommon. Hyperhidrosis and maceration may be present and facilitate dermatophytosis.4,7 Rarely, associated knuckle pads or clubbed digits have been documented.8
Orthohyperkeratosis, acanthosis, papillomatosis Non-epidermolytic (NEPPK) type Bothnia, type Nagashima, type Kimonis, Mal de Meleda (and variant Gamborg Nielsen), Huriez/Howel-Evans/Papillon-Lefèvre/Vohwinkel syndrome, (Greither keratoderma, non-epidermolytic variant), and others
Orthohyperkeratosis with focal parakeratosis, acanthosis, papillomatosis KLICK syndrome, erythrokeratoderma variabilis, HID/KID syndrome
Orthohyperkeratosis with parakeratosis and hypergranulosis with transitional cells Loricrin keratoderma
Widening of intercellular spaces and partial dehiscence of keratinocytes Striate palmoplantar keratoderma (type I, II), diffuse non-specified PPK with DSG1 mutation, Carvajal-Huerta syndrome, McGrath syndrome
The ‘tonotubular’ subtype of PPK is associated with disabling pain on palms.14 Epidermolytic hyperkeratosis with polycyclic psoriasiform plaques is another distinct variant characterized by intermittent flares of fixed polycylic, erythematous, psoriasiform plaques along with diffuse palmoplantar hyperkeratosis.17 A form of diffuse PKK where the keratosis progressively extends to the dorsum of the Achilles tendon, ankles, knee or elbows has been described as Greither keratoderma (keratosis palmoplantaris diffusa transgrediens et progrediens).18 However, not all cases of Greither keratoderma are due to a keratin mutation. The non-epidermolytic variants are discussed below.
Identification of the epidermolytic form of PPK has therapeutic consequences since lesions become inflammatory and erosive upon systemic retinoid therapy.
Epithelia with pale cytoplasm and eosinophilic inclusions Pachyonychia congenita Oculocutaneous tyrosinemia
Depressed epidermis
- with overlying orthohyperkeratotic, focally parakeratotic plaque
Keratosis punctata palmoplantaris type Buschke-Fischer-Bauer Keratosis punctata of palmar creases Marginal papular keratoderma
- with overlaying parakeratotic column
Spiny keratoderma
- with overlying orthohyperkeratotic, focally parakeratotic plaque,
fragmentation and loss of elastic fibers Acrokeratoelastoidosis Costa
Pathogenesis and histologic features Epidermolytic palmoplantar keratoderma was initially mapped to chromosome 17q12-q21, the locus of the type I acidic keratin cluster, where different point mutations of KRT9 encoding keratin 9 were identified. Epidermolytic palmoplantar keratoderma, however, has also been reported to be associated with keratin 1 mutations that map to chromosome 12q11–13, the site of the keratin II genes.9–15 Keratin 1 and 9 are the major structural keratins in the suprabasal keratinocytes of the palmoplantar epidermis. Mutations in KRT9 are associated with more severe manifestations than mutations in KRT1. 10
Most of the keratin mutations affect the central regions of the protein, which are important for filament assembly and stability of the keratin skeleton. As a consequence, tonofilament clumping causes cellular degeneration and disruption, e.g., epidermolytic palmoplantar keratoderma. Mutations in the rod domain are associated with only mild focal signs of epidermolytic
88 Disorders of keratinization
hyperkeratosis in the spinous layer of the palmoplantar epidermis.13 Epidermolytic palmoplantar keratoderma with unusual formation of ‘tonotubular’ filaments is caused by mutations of the 1B rod domain of keratin 1.15,16 Epidermolytic palmoplantar keratoderma is not associated with malignancy, although patients in one large kindred showed a high incidence of breast and ovarian cancer.19 It is now believed that this represented a coincidental cosegregation of a keratin 9 mutation with a BRCA1 mutation on 17q21.2.20
Histologically, there is massive orthohyperkeratosis, hypergranulosis, papillomatosis, and acanthosis accompanied by features of epidermolytic hyperkeratosis in the spinous and granular cell layers with vacuolated
cytoplasm, intracytoplasmic eosinophilic granules, and coarse keratohyalin granules (Figs 3.85 and 3.86). A superficial dermal perivascular lymphohistiocytic infiltrate may sometimes be present. Epidermal spongiosis and vesiculation usually indicates fungal superinfection.
Electron microscopy shows aggregations of keratin filaments and keratin clumps that account for the intracytoplasmic eosinophilic granules as seen by light microscopy. Large areas of the cytoplasm that are devoid of a keratin skeleton explain the vacuolar change. Keratohyalin granules cluster in a random fashion around the keratin aggregates.

Fig. 3.82 Diffuse palmoplantar keratoderma Vörner-Unna-Thost: there is hyperkeratosis affecting the entire sole of the foot. By courtesy of W.A.D. Griffiths, MD, Institute of Dermatology, London, UK.

Fig. 3.83 Diffuse palmoplantar keratoderma Vörner-Unna-Thost: in this patient the palms of the hands were also affected. By courtesy of W.A.D. Griffiths, MD, Institute of Dermatology, London, UK.

Fig. 3.84 Diffuse palmoplantar keratoderma Vörner-Unna-Thost: the border of the lesion is marked by a linear zone of erythema. By courtesy of W.A.D. Griffiths, MD, Institute of Dermatology, London.
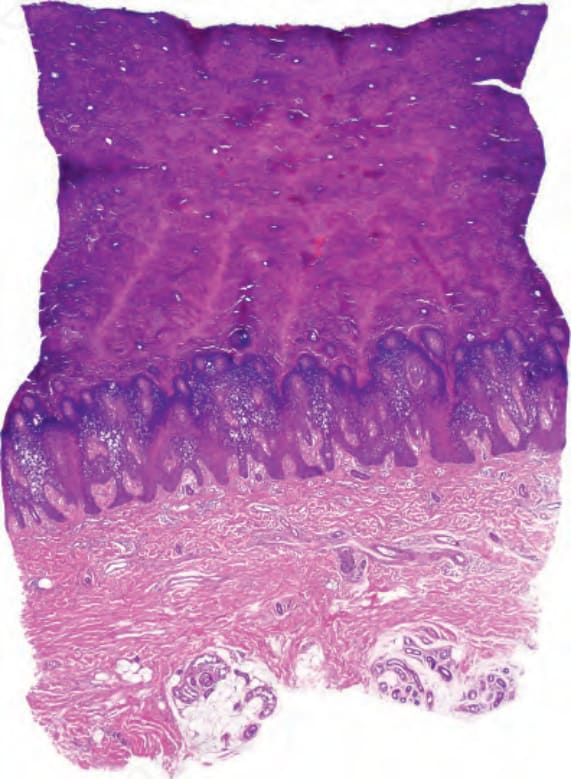
Fig. 3.85 Diffuse palmoplantar keratoderma Vörner-Unna-Thost: scanning view showing massive hyperkeratosis, papillomatosis, and acanthosis.
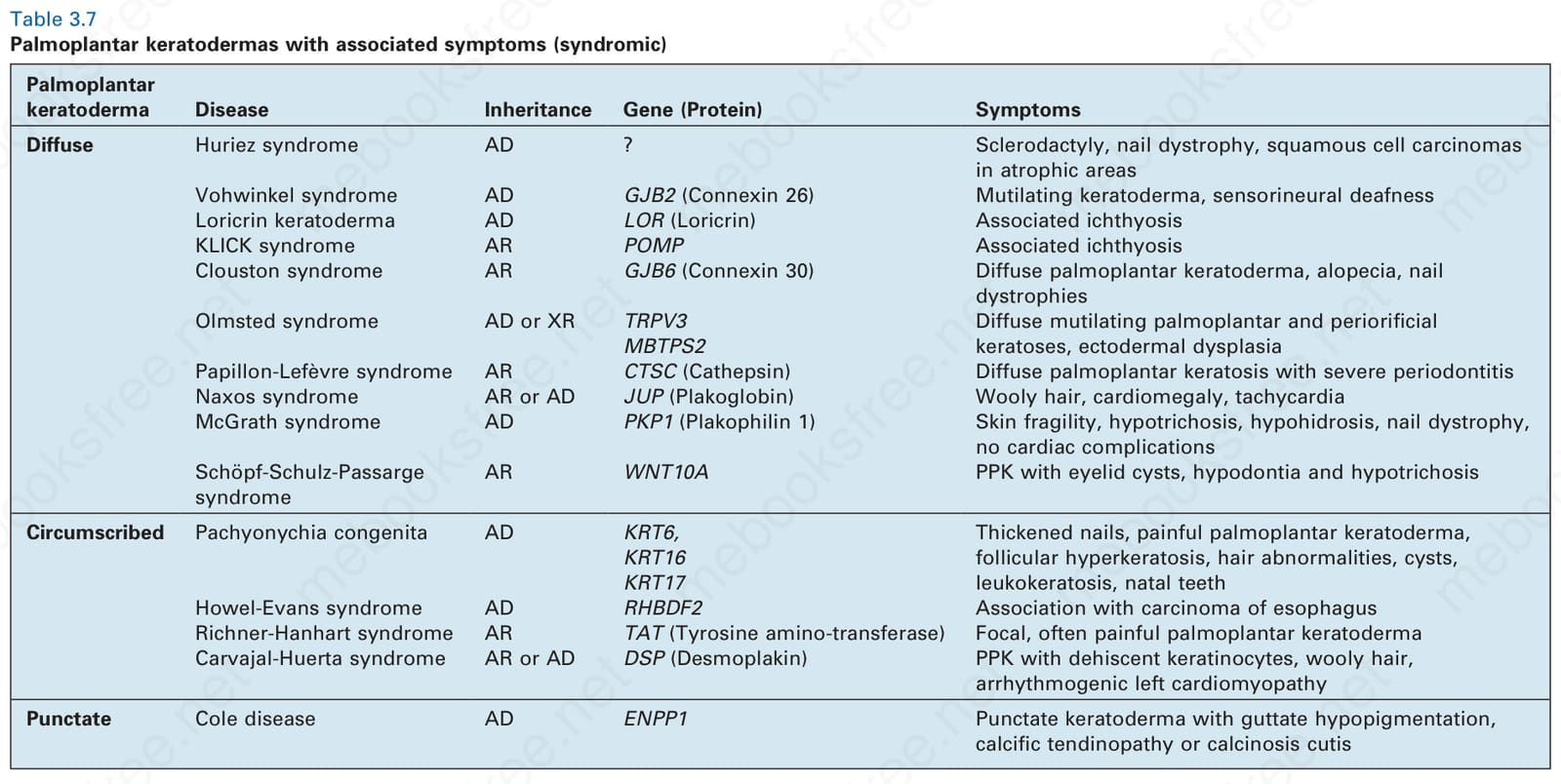
Table 3.7 Palmoplantar keratodermas with associated symptoms (syndromic)
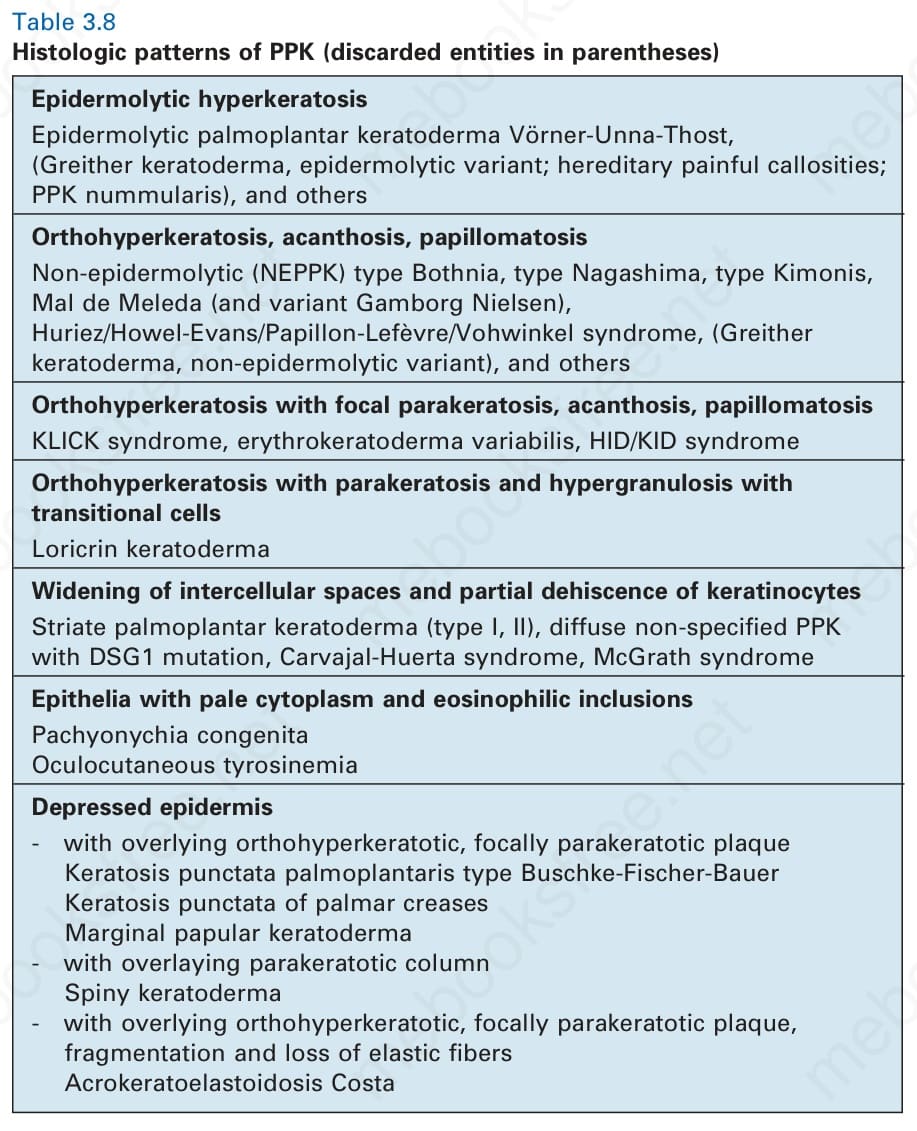
Table 3.8 Histologic patterns of PPK (discarded entities in parentheses)